You might also like
- Cheat Sheet RevisedDocument2 pagesCheat Sheet RevisedUSC Upstate Nursing Coaches100% (3)
- MRN: - Weight: - KG Age: - : Risk/RestraintDocument2 pagesMRN: - Weight: - KG Age: - : Risk/Restraintrustiejade100% (3)
- Brain 1Document1 pageBrain 1Nurse BettyNo ratings yet
- Nursing "Brains" Report Sheet 1Document1 pageNursing "Brains" Report Sheet 1girlywhirl100% (2)
- Medsurg Report SheetDocument1 pageMedsurg Report Sheetjjuplifter100% (3)
- Nurse Report SheetDocument1 pageNurse Report SheetTassos KolliasNo ratings yet
- Student Resource Nurse WorksheetDocument1 pageStudent Resource Nurse WorksheetJerry GNo ratings yet
- Patient Worksheet - MedSurg 2-PatientDocument1 pagePatient Worksheet - MedSurg 2-PatientJerry GNo ratings yet
- Nursing Report Sheet (Revised For Neuro)Document1 pageNursing Report Sheet (Revised For Neuro)HayleyLangley100% (4)
- Nurse Brain Sheet With Shift HoursDocument2 pagesNurse Brain Sheet With Shift HoursLauren Cournoyer Foreman100% (4)
- Nursing Cheat SheetDocument1 pageNursing Cheat SheetMelissa HarndenNo ratings yet
- ChartingDocument1 pageChartingberhanubedassa100% (2)
- Best Nursing Brains 2 Pk.7.15.2013Document3 pagesBest Nursing Brains 2 Pk.7.15.2013Patrica Lynn Kruger67% (6)
- Nursing "Brains" Report Sheet 4Document1 pageNursing "Brains" Report Sheet 4girlywhirl100% (2)
- Med Surg Nurse Brain SheetDocument2 pagesMed Surg Nurse Brain SheetJan Marcus95% (20)
- New Shift Report Sheet 2008Document1 pageNew Shift Report Sheet 2008cutevivesNo ratings yet
- Patient Care Documentation FormDocument1 pagePatient Care Documentation FormJan MarcusNo ratings yet
- Nurse Brain Sheet Half SizeDocument1 pageNurse Brain Sheet Half Sizevsosa624No ratings yet
- Morgan Brain Sheet YayyyDocument2 pagesMorgan Brain Sheet YayyyMorgan NeelyNo ratings yet
- Patient Worksheet - Pediatrics 1-PatientDocument1 pagePatient Worksheet - Pediatrics 1-PatientJerry G100% (1)
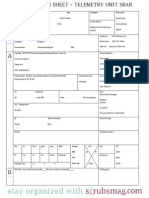
- Nurse Brain Sheet Telemetry Unit SBARDocument1 pageNurse Brain Sheet Telemetry Unit SBARashdmb217No ratings yet
- Nursing SheetDocument1 pageNursing Sheetseaturtles505100% (1)
- Nurse Brain Sheet New Shift ReportDocument1 pageNurse Brain Sheet New Shift ReportRosemaryCastroNo ratings yet
- Daily Nursing AssessmentDocument2 pagesDaily Nursing Assessmentkiku_laiNo ratings yet
- Brain SheetDocument1 pageBrain SheetcutevivesNo ratings yet
- Patient admission details and care plansDocument2 pagesPatient admission details and care plansirish274No ratings yet
- Nurse's Brain SheetDocument1 pageNurse's Brain SheetJan MarcusNo ratings yet
- Blank Basic Nursing Physical AssessmentDocument1 pageBlank Basic Nursing Physical AssessmentAmeliaM100% (3)
- Patient Worksheet - MedSurg 3-PatientDocument1 pagePatient Worksheet - MedSurg 3-PatientJerry G100% (1)
- Fullsize SBAR Report SheetDocument1 pageFullsize SBAR Report SheetShane LambertNo ratings yet
- ICU Nurse Report SheetDocument1 pageICU Nurse Report SheetPuteri Hutami50% (4)
- Nurse BrainDocument2 pagesNurse BrainSam VinikNo ratings yet
- Nurse Report Sheet SBARDocument4 pagesNurse Report Sheet SBARBryan Nguyen50% (2)
- ICU Nursing Report SheetDocument2 pagesICU Nursing Report Sheetthenekoling100% (2)
- Nurse Brain Sheet Telemetry Unit SBARDocument1 pageNurse Brain Sheet Telemetry Unit SBARvsosa624No ratings yet
- Nursing "Brains" Report Sheet 3Document1 pageNursing "Brains" Report Sheet 3girlywhirlNo ratings yet
- Physical Assessment Charting For NursingDocument7 pagesPhysical Assessment Charting For NursingChristine Schroeder92% (13)
- ICU RN Report SheetDocument2 pagesICU RN Report SheetKatie Hecker100% (1)
- My Brain SheetDocument2 pagesMy Brain Sheetkellyae100% (1)
- Nursing Report SheetDocument2 pagesNursing Report SheetsarahNo ratings yet
- 5 PT Med Surg Brain SheetDocument2 pages5 PT Med Surg Brain SheetJan Marcus100% (2)
- Suggested Word List For DocumentationDocument1 pageSuggested Word List For Documentationjkbills100% (6)
- Comprehensive physical exam findingsDocument3 pagesComprehensive physical exam findingsCatherine Drew Sims100% (6)
- Sbar 2Document2 pagesSbar 2Nurse Betty100% (3)
- Head To Toe Assessment Guide PDFDocument6 pagesHead To Toe Assessment Guide PDFTashaNo ratings yet
- Nurse Brain Sheet 12 Hour Day Night RotationDocument1 pageNurse Brain Sheet 12 Hour Day Night Rotationvsosa624No ratings yet
- Comprehensive patient assessmentDocument3 pagesComprehensive patient assessmentAmber Miner TaymanNo ratings yet
- EKG Basics1Document16 pagesEKG Basics1Jamie Lemons100% (1)
- Secrets From The World's Most Productive Nurse PractitionerFrom EverandSecrets From The World's Most Productive Nurse PractitionerNo ratings yet
- The 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsFrom EverandThe 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsNo ratings yet
- Nursing care process in patients with chronic obstructive pulmonary diseaseFrom EverandNursing care process in patients with chronic obstructive pulmonary diseaseNo ratings yet
- MEDICAL-SURGICAL NURSE: Passbooks Study GuideFrom EverandMEDICAL-SURGICAL NURSE: Passbooks Study GuideNo ratings yet
- So, You Wanna Be A Travel Nurse?: An Insider's Guide to Getting StartedFrom EverandSo, You Wanna Be A Travel Nurse?: An Insider's Guide to Getting StartedRating: 5 out of 5 stars5/5 (1)
- Dimensional Analysis For Nursing StudentsFrom EverandDimensional Analysis For Nursing StudentsNo ratings yet
- 30 Day Preparedness List As Table - Flutrackers Dot ComDocument2 pages30 Day Preparedness List As Table - Flutrackers Dot ComgirlywhirlNo ratings yet
- 30 Day Preparedness List As TableDocument2 pages30 Day Preparedness List As TablegirlywhirlNo ratings yet
- Nursing "Brains" Report Sheet 4Document1 pageNursing "Brains" Report Sheet 4girlywhirl100% (2)
- Nursing "Brains" Report Sheet 3Document1 pageNursing "Brains" Report Sheet 3girlywhirlNo ratings yet
- Nursing "Brains" Report Sheet 3Document1 pageNursing "Brains" Report Sheet 3girlywhirlNo ratings yet
- Nursing "Brains" Report Sheet 4Document1 pageNursing "Brains" Report Sheet 4girlywhirl100% (2)
- Nursing "Brains" Report Sheet 2Document1 pageNursing "Brains" Report Sheet 2girlywhirl100% (4)