You might also like
- Eating DisordersDocument45 pagesEating DisordersJasmin JacobNo ratings yet
- NCP Anorexia NervosaDocument7 pagesNCP Anorexia NervosaW'ton Borbe83% (6)
- Generalized Anxiety DisorderDocument13 pagesGeneralized Anxiety Disorderapi-3797941100% (1)
- Obsessive Compulsive DisorderDocument7 pagesObsessive Compulsive Disorderapi-379794190% (10)
- Bulimia Nervosa: Elmeida EffendyDocument14 pagesBulimia Nervosa: Elmeida EffendyputriNo ratings yet
- Major Depressive Disorder: Presented By: Justin Darrell A. SALACUPDocument15 pagesMajor Depressive Disorder: Presented By: Justin Darrell A. SALACUPJoana Mikee Rasay100% (1)
- Xanax Drug CardDocument3 pagesXanax Drug Cardnasir khanNo ratings yet
- Post Traumatic Stress DisorderDocument23 pagesPost Traumatic Stress Disorderapi-379794175% (4)
- Pathophysiology of Bipolar DisorderDocument1 pagePathophysiology of Bipolar DisorderbeshyNo ratings yet
- Anorexia Nervosa Handbook ChapterDocument17 pagesAnorexia Nervosa Handbook ChapterOchaNo ratings yet
- Major Depression - Dysthymic DisorderDocument28 pagesMajor Depression - Dysthymic Disorderapi-3797941No ratings yet
- Mental Status ExaminationDocument4 pagesMental Status ExaminationZamranos67% (3)
- Nursing Care Plan For A Patient With Bipolar DisorderDocument20 pagesNursing Care Plan For A Patient With Bipolar Disordermjk2100% (4)
- Patient Education schiZOphreniaDocument2 pagesPatient Education schiZOphreniarinkai13100% (1)
- Major Depressive DisorderDocument3 pagesMajor Depressive Disorderregz1No ratings yet
- Obsessive Compulsive DisorderDocument14 pagesObsessive Compulsive Disorderfrancis00090100% (1)
- Activity IntoleranceDocument6 pagesActivity IntoleranceDenvEr CabaniLlasNo ratings yet
- Bipolar 2 Disorder Case StudyDocument11 pagesBipolar 2 Disorder Case Studyapi-402293970100% (2)
- ND - Risk For SuicideDocument3 pagesND - Risk For SuicideHu Dawi100% (1)
- Aripiprazole Guide for NursesDocument4 pagesAripiprazole Guide for NursesAP TOROBX100% (1)
- Disturbed Sleep Pattern in Bipolar ClientDocument2 pagesDisturbed Sleep Pattern in Bipolar ClientJermaine Anne MadayagNo ratings yet
- HaldolDocument2 pagesHaldolKatie McPeek100% (2)
- Pathophysiology of Bipolar 1 DisorderDocument1 pagePathophysiology of Bipolar 1 DisorderMark Cau Meran100% (3)
- Pathophysiology of Bipolar DisorderDocument1 pagePathophysiology of Bipolar DisorderGab Abalos100% (2)
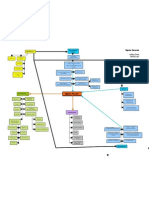
- Bipolar Disorder Concept MapDocument1 pageBipolar Disorder Concept Mapashleydean100% (1)
- Bipolar NCPDocument2 pagesBipolar NCPBrenn Marie RamosNo ratings yet
- Binge Eating DisorderDocument11 pagesBinge Eating DisorderShorli8350% (2)
- Girl InterruptedDocument17 pagesGirl Interruptedapi-337713711100% (1)
- Drug Study HaldolDocument2 pagesDrug Study HaldolGracia EvangelistaNo ratings yet
- ProzacDocument1 pageProzacE100% (1)
- NCP For BipolarDocument14 pagesNCP For BipolarSheana Tmpl100% (1)
- Undifferentiated SchizophreniaDocument26 pagesUndifferentiated SchizophreniaVictor Shon100% (1)
- Mental Status ExaminationDocument10 pagesMental Status Examinationlatasha deshmukhNo ratings yet
- Case Study Psychia Bipolar 2Document57 pagesCase Study Psychia Bipolar 2Joule PeirreNo ratings yet
- Mental Status Examination - Bring To LectureDocument6 pagesMental Status Examination - Bring To LectureJae ChoiNo ratings yet
- SchizophreniaDocument27 pagesSchizophreniacadpsy100% (3)
- Eating Disorders TreatmentDocument14 pagesEating Disorders Treatmentapi-245243640No ratings yet
- Outline of Mental Status ExaminationDocument10 pagesOutline of Mental Status ExaminationMohammed Hosen100% (1)
- 2019 Psych Updated 2Document9 pages2019 Psych Updated 2Nae OrdanozoNo ratings yet
- Nursing Care Guide for Cushing's SyndromeDocument2 pagesNursing Care Guide for Cushing's Syndromerngeneral50% (6)
- Ineffective CopingDocument14 pagesIneffective CopingNdel LindaNo ratings yet
- Ocd PsychopathologyDocument14 pagesOcd PsychopathologyelvinegunawanNo ratings yet
- A Grand Case UgibDocument84 pagesA Grand Case UgibAdrianne Kricia100% (2)
- Colace (Docusate Sodium)Document1 pageColace (Docusate Sodium)E100% (1)
- GRP 4 CLO 2 Concept Map PT 1 PDFDocument14 pagesGRP 4 CLO 2 Concept Map PT 1 PDFMaria Lyn Ocariza ArandiaNo ratings yet
- Individualized Teaching Plan for Diabetes ManagementDocument2 pagesIndividualized Teaching Plan for Diabetes ManagementNicole LichtenbergNo ratings yet
- Librium ChlordiazepoxideDocument2 pagesLibrium ChlordiazepoxideENo ratings yet
- HoplessnessDocument16 pagesHoplessnessHamza IshtiaqNo ratings yet
- The Pathophysiology of Schizophrenia DisordersDocument16 pagesThe Pathophysiology of Schizophrenia DisordersElsya ApriliaNo ratings yet
- NCP & Discharge PlanningDocument12 pagesNCP & Discharge PlanningStephanie Mae Amoylen OdchigueNo ratings yet
- NCP Eating Disorders ObesityDocument20 pagesNCP Eating Disorders ObesityW'ton BorbeNo ratings yet
- Anorexia Nervosa/Bulimia Nervosa: Dsm-IvDocument5 pagesAnorexia Nervosa/Bulimia Nervosa: Dsm-IvNicolo Paulo TabiraraNo ratings yet
- Anorexia Nervosa - Bulimia NervosaDocument17 pagesAnorexia Nervosa - Bulimia Nervosaapi-37642150% (1)
- Eating Disorder Types and TreatmentDocument47 pagesEating Disorder Types and TreatmentRujuta BaramateNo ratings yet
- Eating Disorder PPT by Shreyasi MittalDocument35 pagesEating Disorder PPT by Shreyasi MittalPrachi gattaniNo ratings yet
- Anorexia NervosaDocument8 pagesAnorexia NervosaSondos HANo ratings yet
- Eating DisordersDocument71 pagesEating DisordersMonina JonesNo ratings yet
- Eating DisordersDocument6 pagesEating DisordersCharisse Lutero100% (1)
- 12B. EatingDisorders - 01Document57 pages12B. EatingDisorders - 01Rubilyn SumayloNo ratings yet
- Eating Disorders 1Document11 pagesEating Disorders 1karlaNo ratings yet
- Somatoform DisordersDocument18 pagesSomatoform Disordersapi-376421589% (9)
- STIMULANTSDocument13 pagesSTIMULANTSapi-3764215No ratings yet
- Substance Dependence - Abuse RehabilitationDocument19 pagesSubstance Dependence - Abuse Rehabilitationapi-3764215No ratings yet
- Premenstrual Dysphoric DisorderDocument11 pagesPremenstrual Dysphoric Disorderapi-3764215No ratings yet
- Schizoaffective DisorderDocument8 pagesSchizoaffective Disorderapi-3797941100% (8)
- SchizophreniaDocument36 pagesSchizophreniaapi-379794183% (6)
- Sexual Dysfunctions and ParaphiliasDocument12 pagesSexual Dysfunctions and Paraphiliasapi-3797941100% (3)
- Psychological Factors Affecting Medical ConditionDocument17 pagesPsychological Factors Affecting Medical Conditionapi-3797941100% (3)
- Panic Disorder PhobiasDocument9 pagesPanic Disorder Phobiasapi-3797941No ratings yet
- Passive - Aggressive Personality DisorderDocument9 pagesPassive - Aggressive Personality DisorderCay SevillaNo ratings yet
- Post Traumatic Stress DisorderDocument23 pagesPost Traumatic Stress Disorderapi-379794175% (4)
- PARENTING - Growth - Promoting RelationshipDocument13 pagesPARENTING - Growth - Promoting Relationshipapi-3764215No ratings yet
- Pervasive Developmental DisordersDocument11 pagesPervasive Developmental Disordersapi-3797941No ratings yet
- Problems Related To Abuse or NeglectDocument25 pagesProblems Related To Abuse or Neglectapi-3797941100% (5)
- Oppositional Defiant DisorderDocument9 pagesOppositional Defiant Disorderapi-3764215100% (3)
- Dementia of The Alzheimers Type - Vascular DementiaDocument31 pagesDementia of The Alzheimers Type - Vascular Dementiaapi-3797941No ratings yet
- Delusional DisorderDocument12 pagesDelusional Disorderapi-3797941100% (1)
- Major Depression - Dysthymic DisorderDocument27 pagesMajor Depression - Dysthymic DisorderCay SevillaNo ratings yet
- Hallucinogen Phencyclidine and Cannabis - Related DisordersDocument13 pagesHallucinogen Phencyclidine and Cannabis - Related Disordersapi-3797941No ratings yet
- Bipolar DisordersDocument18 pagesBipolar DisordersBSNNursing101No ratings yet
- Gender Identity DisorderDocument12 pagesGender Identity Disorderapi-3797941100% (1)
- Elimination Disorders Enuresis SisDocument9 pagesElimination Disorders Enuresis Sisapi-3797941100% (1)
- ObesityDocument12 pagesObesityapi-3797941No ratings yet
- DepressantsDocument8 pagesDepressantsapi-3797941No ratings yet
- Conduct DisorderDocument20 pagesConduct Disorderapi-3764215100% (1)
- Borderline Personality DisorderDocument14 pagesBorderline Personality DisorderBSNNursing101No ratings yet
- Dissociative DisordersDocument17 pagesDissociative Disordersapi-3797941100% (4)
- Dementia Due To Hiv DiseaseDocument13 pagesDementia Due To Hiv DiseaseCay SevillaNo ratings yet
- Adult Nutrition Assessment Tutorial 2012Document9 pagesAdult Nutrition Assessment Tutorial 2012Dariana floresNo ratings yet
- Nursing Practice VDocument11 pagesNursing Practice Vapi-3718174No ratings yet
- ASPEN Consensus Recommendations For RefeedingDocument18 pagesASPEN Consensus Recommendations For RefeedingCLAUDIA PATRICIA AGUADO QUINTERONo ratings yet
- Inglés Junio 1-5 PDFDocument6 pagesInglés Junio 1-5 PDFJuan DiegoNo ratings yet
- Kearney Ch5Document14 pagesKearney Ch5Savio RebelloNo ratings yet
- 4 2 Fill in Notes PearsonDocument14 pages4 2 Fill in Notes PearsonMelanieNo ratings yet
- CD 13,14,15-10E1 With KeyDocument12 pagesCD 13,14,15-10E1 With KeyĐinh Nguyễn Quỳnh ChâuNo ratings yet
- Cultural Factors Behind Rising Eating Disorders in JapanDocument39 pagesCultural Factors Behind Rising Eating Disorders in JapanVictória NamurNo ratings yet
- Etextbook PDF For Abnormal Psychology 2nd Edition by Robin S RosenbergDocument62 pagesEtextbook PDF For Abnormal Psychology 2nd Edition by Robin S Rosenbergoscar.gokey720100% (43)
- Nutrition Management For Eating DisordersDocument3 pagesNutrition Management For Eating DisordersliggiedyNo ratings yet
- Edi PresentationDocument20 pagesEdi Presentationapi-12257981100% (2)
- 2019 - Enhanced Cognitive Behavioral Therapy For Adolescents With Anorexia Nervosa - Outcomes and Predictors of Change in A Real-World SettingDocument6 pages2019 - Enhanced Cognitive Behavioral Therapy For Adolescents With Anorexia Nervosa - Outcomes and Predictors of Change in A Real-World SettingpabobadillaNo ratings yet
- GIT Anorexia PharmaPedia PharmaGatesDocument10 pagesGIT Anorexia PharmaPedia PharmaGatesIslam FawzyNo ratings yet
- Health Issues Facing Adolescents in IndiaDocument51 pagesHealth Issues Facing Adolescents in IndiaJerome Manaig SueltoNo ratings yet
- Bios ClassificationDocument112 pagesBios ClassificationNeseriani AndersonNo ratings yet
- Mairs R Et Al 2016Document8 pagesMairs R Et Al 2016Camilla ValeNo ratings yet
- Factors Leading to AnorexiaDocument7 pagesFactors Leading to AnorexiaEsther XiaToong LauNo ratings yet
- Exploring Feeding Difficulties in Children The Generosity of Acceptance by Gianna Polacco WilliamsDocument262 pagesExploring Feeding Difficulties in Children The Generosity of Acceptance by Gianna Polacco WilliamsrichardNo ratings yet
- From Disorder To Political ActionDocument16 pagesFrom Disorder To Political ActionCamila OrellanaNo ratings yet
- CML Research EssayDocument7 pagesCML Research Essayapi-358692407No ratings yet
- Eating Disorders (Barlow and Durand - Pp. 269 - 295)Document27 pagesEating Disorders (Barlow and Durand - Pp. 269 - 295)Monina JonesNo ratings yet
- Anorexia NervoasaDocument31 pagesAnorexia NervoasaRaluca Vişovan100% (2)
- 3th Year Residency 2Document17 pages3th Year Residency 2Spacetoon DaysNo ratings yet
- Reducing Anxiety Through Music Therapy at An Outpatient Eating Disorder Recovery Service PDFDocument10 pagesReducing Anxiety Through Music Therapy at An Outpatient Eating Disorder Recovery Service PDFAlessandroBeniniNo ratings yet
- Eating DisorderdDocument17 pagesEating DisorderdAndreea NicolaeNo ratings yet
- Literature ReviewDocument4 pagesLiterature ReviewfebiwNo ratings yet
- The Secrets of A Master Practitioner: Energy MedicineDocument14 pagesThe Secrets of A Master Practitioner: Energy MedicineMarco Sughatto100% (1)
- Reed Et Al (1991) - Development and Validation of The Physical Appearance State and Trait Anxiety Scale (PASTAS)Document10 pagesReed Et Al (1991) - Development and Validation of The Physical Appearance State and Trait Anxiety Scale (PASTAS)nalaNo ratings yet
- Crozier Revised 2010 P02568 The History of PsychiatryDocument11 pagesCrozier Revised 2010 P02568 The History of Psychiatrygae24341No ratings yet
- Loving Them To Death The Anorexic and Her Objects-1Document14 pagesLoving Them To Death The Anorexic and Her Objects-1Gabriela CiucuNo ratings yet