You might also like
- Drugs Used in ChemotherapyDocument4 pagesDrugs Used in ChemotherapyArman Leal Bernardo100% (1)
- Nursing OncologyDocument131 pagesNursing Oncologyapi-3818438100% (5)
- Oncology NursingDocument120 pagesOncology Nursingstuffednurse100% (1)
- Care of Patients With CancerDocument57 pagesCare of Patients With CancerAyessa Yvonne PanganibanNo ratings yet
- Cancer NursingDocument53 pagesCancer Nursingfairwoods100% (1)
- Hematologic SystemDocument81 pagesHematologic Systemseigelystic100% (23)
- Testicular Cancer Nursing ManagementDocument33 pagesTesticular Cancer Nursing ManagementCheeBrendaNo ratings yet
- Oncology Nursing OverviewDocument12 pagesOncology Nursing OverviewTiffany Luv AdriasNo ratings yet
- Breast Cancer Case Study: Answers For LifeDocument4 pagesBreast Cancer Case Study: Answers For LifeFaye Mie VelascoNo ratings yet
- Nursing Care of Patients Receiving Chemotherapy Ranjita Rajesh Lecturer People's College of Nursing BhopalDocument55 pagesNursing Care of Patients Receiving Chemotherapy Ranjita Rajesh Lecturer People's College of Nursing BhopalFayizatul AkmarNo ratings yet
- B. Pathophysiology: Clinical Aspects of Cancer DiagnosisDocument10 pagesB. Pathophysiology: Clinical Aspects of Cancer DiagnosisAbigael Patricia GutierrezNo ratings yet
- Oncology Nursing - OverviewDocument137 pagesOncology Nursing - OverviewMae DacerNo ratings yet
- NCLEX OncologyDocument2 pagesNCLEX OncologyJenniDamuNo ratings yet
- Nursing Care of The Client With CancerDocument15 pagesNursing Care of The Client With CancerAlvin M Alcayno0% (1)
- Mastectomy patient chemotherapy side effects NCLEX reviewDocument4 pagesMastectomy patient chemotherapy side effects NCLEX reviewTinNo ratings yet
- Safe Handling Chemotherapy DrugsDocument62 pagesSafe Handling Chemotherapy DrugsKaterina Georgiadi KalogianniNo ratings yet
- Wound AssessmentDocument19 pagesWound Assessmentdrsonuchawla100% (1)
- Oncology Nursing Part 1 2Document51 pagesOncology Nursing Part 1 2fleur harrisonNo ratings yet
- Oncology Ang Pain - 150itemsDocument23 pagesOncology Ang Pain - 150itemsJoms Kim MinaNo ratings yet
- 2016 ASCO - ONS Chemo Standards PDFDocument13 pages2016 ASCO - ONS Chemo Standards PDFSindu SaiNo ratings yet
- Oncology QuestionsDocument3 pagesOncology QuestionsWilma BaludoNo ratings yet
- Chemotherapy Guidelines NurseDocument82 pagesChemotherapy Guidelines NurseochanpsikNo ratings yet
- Chemotherapy - Alkylating AgentsDocument33 pagesChemotherapy - Alkylating AgentsNolan100% (1)
- Nursing: TraditionalDocument21 pagesNursing: TraditionalVincent Ranara SabornidoNo ratings yet
- Prevent Pressure Ulcers with Proper Skin Care, Repositioning and Support SurfacesDocument6 pagesPrevent Pressure Ulcers with Proper Skin Care, Repositioning and Support SurfacesasuratosNo ratings yet
- Oncology Nursing Handouts 1Document8 pagesOncology Nursing Handouts 1pauchanmnlNo ratings yet
- Oncology Nursing CareDocument18 pagesOncology Nursing CareMichael Urrutia100% (1)
- Nursing Portfolio - Clinical ExemplarDocument6 pagesNursing Portfolio - Clinical Exemplarapi-304645018100% (3)
- Chemotherapy and Biotherapy Hypersensitivity Reactions: Christine E. Coyle, RN, BSN, OCNDocument55 pagesChemotherapy and Biotherapy Hypersensitivity Reactions: Christine E. Coyle, RN, BSN, OCNRakesh MishraNo ratings yet
- Principles of Oncology NursingDocument12 pagesPrinciples of Oncology NursingДария Коваленко100% (1)
- Breast Cancer!!!Document24 pagesBreast Cancer!!!twahyuningsih_16No ratings yet
- Oncology Case StudyDocument8 pagesOncology Case Studyapi-273522923No ratings yet
- Oncology-Study of Cancer Cellular AbberationDocument43 pagesOncology-Study of Cancer Cellular AbberationIrwan M. IskoberNo ratings yet
- Nursing OncologyDocument208 pagesNursing OncologyfelxhuNo ratings yet
- Cervical Cancer: Causes, Symptoms, Diagnosis and TreatmentDocument59 pagesCervical Cancer: Causes, Symptoms, Diagnosis and TreatmentClaudiaNathaliaNo ratings yet
- Chemotherapy Treatment OverviewDocument145 pagesChemotherapy Treatment OverviewShweta MishraNo ratings yet
- Oncology NursingDocument10 pagesOncology NursingCham Rafaela Conese100% (3)
- Oncology NotesDocument7 pagesOncology Notesaurezea100% (1)
- BREAST CANCERppt NCM 106 Updated July 7Document103 pagesBREAST CANCERppt NCM 106 Updated July 7sweet25chocolat100% (1)
- Management of CholeraDocument69 pagesManagement of CholeraNatalia LawrenceNo ratings yet
- Chemo MedsDocument17 pagesChemo MedsSophia Smartz100% (1)
- Surgical Treatment For BREAST CANCERDocument5 pagesSurgical Treatment For BREAST CANCERJericho James TopacioNo ratings yet
- OncologyDocument8 pagesOncologyJhiLy 사랑의 케빈 우No ratings yet
- Oncology NursingDocument158 pagesOncology NursingHebsiba PonnayyanNo ratings yet
- Course Specification Emergency NursingDocument6 pagesCourse Specification Emergency NursingWael LotfyNo ratings yet
- Oncology Nursing: New and Indispensable Resources inDocument11 pagesOncology Nursing: New and Indispensable Resources inAnonymous WLibJwGgNo ratings yet
- Oncology Nursing HandoutsDocument7 pagesOncology Nursing HandoutsShandz de Rosas100% (1)
- Chapter 6 Cancer PrepU QuestionsDocument7 pagesChapter 6 Cancer PrepU QuestionsKevin ClarkNo ratings yet
- NCLEX Review Oncology NursingDocument8 pagesNCLEX Review Oncology NursingJunjun R AquinoNo ratings yet
- Chemotherapeutic DrugsDocument4 pagesChemotherapeutic DrugsEditor IJTSRDNo ratings yet
- M.SC Nursing Syllabus Revised 2018 - 19-23082019-1Document344 pagesM.SC Nursing Syllabus Revised 2018 - 19-23082019-1Divya ToppoNo ratings yet
- Oncology Handouts PDFDocument21 pagesOncology Handouts PDFPhilip Simangan100% (1)
- Management of Tuberculosis: A guide for clinicians (eBook edition)From EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)No ratings yet
- Pass the PSB! Complete Health Occupation Aptitude Test (PSB) study guide and practice test questionsFrom EverandPass the PSB! Complete Health Occupation Aptitude Test (PSB) study guide and practice test questionsNo ratings yet
- Necrotizing Fasciitis, (Flesh Eating Disease) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandNecrotizing Fasciitis, (Flesh Eating Disease) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Pleurisy, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandPleurisy, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- COMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideFrom EverandCOMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideNo ratings yet
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsNo ratings yet
- TC Registration National Guard FormDocument3 pagesTC Registration National Guard Formbrigette_lagatNo ratings yet
- KI DS Shoe SI ZE ChartDocument1 pageKI DS Shoe SI ZE Chartbrigette_lagatNo ratings yet
- Our Cats 02 2013Document84 pagesOur Cats 02 2013brigette_lagatNo ratings yet
- Tips For IeltsDocument8 pagesTips For Ieltsbrigette_lagatNo ratings yet
- Access PortacathDocument3 pagesAccess Portacathbrigette_lagatNo ratings yet
- Ielts Task 2 6 Sample EssaysDocument7 pagesIelts Task 2 6 Sample EssaysSungjin ParkNo ratings yet
- IV Solutions Reference Chart (Uses & Effects)Document1 pageIV Solutions Reference Chart (Uses & Effects)jkbills94% (17)
- Taking Ielts in Saudi ArabiaDocument3 pagesTaking Ielts in Saudi Arabiabrigette_lagatNo ratings yet
- Ielts Speaking Topics & Answers-1.Document17 pagesIelts Speaking Topics & Answers-1.jiguparmar1516100% (8)
- Arabic Medical Terms in English PDFDocument10 pagesArabic Medical Terms in English PDFnarswiponshistoryan77% (22)
- Physical exam findings for medical transcriptionDocument34 pagesPhysical exam findings for medical transcriptionbrigette_lagatNo ratings yet
- Ob BulletsDocument8 pagesOb Bulletsbrigette_lagatNo ratings yet
- IELTS WritingDocument5 pagesIELTS Writingbrigette_lagatNo ratings yet
- MTQUIZDocument89 pagesMTQUIZbrigette_lagatNo ratings yet
- What Is Medical TranscriptionDocument97 pagesWhat Is Medical Transcriptionbrigette_lagatNo ratings yet
- IeltsDocument22 pagesIeltsbrigette_lagatNo ratings yet
- IELTS WritingDocument5 pagesIELTS Writingbrigette_lagatNo ratings yet
- International Rice Research Newsletter Vol.8 No.3Document24 pagesInternational Rice Research Newsletter Vol.8 No.3ccquintosNo ratings yet
- White Blood CorpusclesDocument25 pagesWhite Blood CorpusclesEricaNo ratings yet
- Sanders C04Document38 pagesSanders C04Vo UyNo ratings yet
- NEZUKODocument8 pagesNEZUKOLeonel AguilarNo ratings yet
- Monosaccharides: AlpineDocument12 pagesMonosaccharides: AlpineReigner Jay B. EscartinNo ratings yet
- Pathophysiology of Small Cell Lung CancerDocument2 pagesPathophysiology of Small Cell Lung CancerChristine Pialan SalimbagatNo ratings yet
- 1 s2.0 S0923181121000840 MainDocument16 pages1 s2.0 S0923181121000840 Mainleon4009No ratings yet
- PhysioEx Exercise 3-123Document16 pagesPhysioEx Exercise 3-123NicoleNo ratings yet
- Toxoplasma GondiiDocument40 pagesToxoplasma GondiiNeelam Joshi100% (2)
- FlatwormsDocument19 pagesFlatwormsanon :)No ratings yet
- Epidural and Spinal AnesthesiaDocument86 pagesEpidural and Spinal Anesthesiasarguss1471% (7)
- OSPE 3rd Prof Microscopic Slide of Breast BiopsyDocument144 pagesOSPE 3rd Prof Microscopic Slide of Breast BiopsyMuhammadShahzadNo ratings yet
- Satanism and Power Meditation - 7Document241 pagesSatanism and Power Meditation - 7Luis Lopez100% (6)
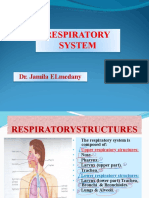
- Respiratory SystemhjhuDocument23 pagesRespiratory SystemhjhuSara ANo ratings yet
- The Fundamental Unit of Life To Improvement in Food Resources ChaptersDocument104 pagesThe Fundamental Unit of Life To Improvement in Food Resources ChaptersSARANSH oPNo ratings yet
- Photosynthesis Science Presentation in Green Beige Illustrative Style - 20230920 - 192536 - 0000Document11 pagesPhotosynthesis Science Presentation in Green Beige Illustrative Style - 20230920 - 192536 - 0000Rei B.XNo ratings yet
- AIIMS SR JULY 2015 PROSTHODONTICS REVIEWDocument34 pagesAIIMS SR JULY 2015 PROSTHODONTICS REVIEWArjun NarangNo ratings yet
- Lockwood & Co. #4 - Creeping Shadow ExcerptDocument17 pagesLockwood & Co. #4 - Creeping Shadow Excerptmsreeat67% (3)
- Encyclopedia of Biological Chemistry - Vol - 1Document895 pagesEncyclopedia of Biological Chemistry - Vol - 1aishbiyaNo ratings yet
- Anatomyinnutshel00laug PDFDocument626 pagesAnatomyinnutshel00laug PDFSifu LiceNo ratings yet
- 3505 Test of NormalityDocument4 pages3505 Test of NormalityMohd Zaini AbdullahNo ratings yet
- Screen Sleep Disorders QuestionnaireDocument2 pagesScreen Sleep Disorders QuestionnaireMarivic Sonido100% (1)
- Dubowitz Ballard Exam Gestational AgeDocument4 pagesDubowitz Ballard Exam Gestational AgeDyah Nuriisa ANo ratings yet
- Lesson PlanDocument10 pagesLesson Planlloyd.villavertNo ratings yet
- General Principles of Fracture ManagementDocument60 pagesGeneral Principles of Fracture ManagementAdrian Joel Quispe AlataNo ratings yet
- PNLE Sample Test QuestionsDocument12 pagesPNLE Sample Test QuestionsHam-Ham LootNo ratings yet
- Water Is Alive Shellys House Speech PDFDocument9 pagesWater Is Alive Shellys House Speech PDFCyndi Lindenberger100% (1)
- Therapy of Diabetic Neuropathy With MecobalaminDocument29 pagesTherapy of Diabetic Neuropathy With MecobalaminKristina FergusonNo ratings yet
- Chapter 19 Blood 2304Document26 pagesChapter 19 Blood 2304Nishchaya SinghNo ratings yet
- Introduction To Biochemistry: Ms. Jirehkriza G. Suganob General Biology 1Document27 pagesIntroduction To Biochemistry: Ms. Jirehkriza G. Suganob General Biology 1Jcob SntosNo ratings yet