You might also like
- Organ Transplantation Policies and Policy Reforms Presentation Powerpoint FinalDocument22 pagesOrgan Transplantation Policies and Policy Reforms Presentation Powerpoint Finalapi-239990812No ratings yet
- Final Law PaperDocument11 pagesFinal Law Paperapi-233745376No ratings yet
- Student Competency AssessmentDocument10 pagesStudent Competency Assessmentapi-233745376No ratings yet
- PC Breast Symposium Lo ResDocument2 pagesPC Breast Symposium Lo Resapi-233745376No ratings yet
- Ireland Reflection PaperDocument5 pagesIreland Reflection Paperapi-233745376No ratings yet
- Business Plan 2013 SubmissionDocument8 pagesBusiness Plan 2013 Submissionapi-233745376No ratings yet
- Business Plan Breast Program2Document16 pagesBusiness Plan Breast Program2api-233745376100% (1)
- Final IrelandDocument9 pagesFinal Irelandapi-233745376No ratings yet
- Multidisciplinary Thoracic Lung1Document14 pagesMultidisciplinary Thoracic Lung1api-233745376No ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5782)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Test Bank For Safe Maternity Pediatric Nursing Care 1st Edition Luanne Linnard Palmer Gloria Haile Coats 2Document5 pagesTest Bank For Safe Maternity Pediatric Nursing Care 1st Edition Luanne Linnard Palmer Gloria Haile Coats 2George Hogan100% (25)
- Community Health Nursing 1 Session # 2: Lesson Preview/ReviewDocument2 pagesCommunity Health Nursing 1 Session # 2: Lesson Preview/ReviewTrexie MarcianoNo ratings yet
- FDA Industry Guidance For Size Shape PhysicalDocument11 pagesFDA Industry Guidance For Size Shape PhysicalAhmed AliNo ratings yet
- Methodical Instructions: For The Practical Classes in Pharmacology TopicDocument3 pagesMethodical Instructions: For The Practical Classes in Pharmacology TopicSahil SainiNo ratings yet
- Rapido DanielDocument28 pagesRapido DanielzalikhaNo ratings yet
- Euthanasia: Hidayatullah National Law University, Raipur, ChhattisgarhDocument22 pagesEuthanasia: Hidayatullah National Law University, Raipur, ChhattisgarhAtul Agrawal100% (1)
- Rabia Poster ComposrDocument1 pageRabia Poster ComposrRabia TinnaNo ratings yet
- Republic of The Philippines Department of HealthDocument28 pagesRepublic of The Philippines Department of HealthTimothy AlmeidaNo ratings yet
- Denial Codes 05aug2020Document9 pagesDenial Codes 05aug2020naharmampillyNo ratings yet
- Donation Pros and ConsDocument8 pagesDonation Pros and Consapi-283648835No ratings yet
- Ten Tips For First Year of RecoveryDocument5 pagesTen Tips For First Year of RecoveryTratament DependenteNo ratings yet
- Ultrasound TechnicianDocument2 pagesUltrasound Technicianapi-76827299No ratings yet
- Usp Review AlbuterolDocument82 pagesUsp Review Albuterolsrayu2603No ratings yet
- Tutorial 4 - Pain ManagementDocument5 pagesTutorial 4 - Pain ManagementSNo ratings yet
- 6 Metronidazole Drug StudyDocument4 pages6 Metronidazole Drug Studyshadow gonzalezNo ratings yet
- A Five-Factor Model of Psychosis With The Mmpi-2-RfDocument49 pagesA Five-Factor Model of Psychosis With The Mmpi-2-RfskafonNo ratings yet
- Research ProposalDocument4 pagesResearch ProposalAmar GandhiNo ratings yet
- Large Intestine Pattern Differentiation in Chinese MedicineDocument6 pagesLarge Intestine Pattern Differentiation in Chinese MedicineFinderlucian Lucian100% (1)
- Pharmacists' Patient Care Process Provides ConsistencyDocument19 pagesPharmacists' Patient Care Process Provides ConsistencyMuh Fadli HusinNo ratings yet
- Due Date Calculator: Are You Counting Weeks, Months and Trimesters? Use Our Due Date Birthday!Document6 pagesDue Date Calculator: Are You Counting Weeks, Months and Trimesters? Use Our Due Date Birthday!Sanjay Kumar SanjuNo ratings yet
- Nursing Crib Com NURSING CARE PLAN Spontaneous AbortionDocument2 pagesNursing Crib Com NURSING CARE PLAN Spontaneous AbortionJustin PasaronNo ratings yet
- A Study On Effectiveness of Low Level Laser Therapy and Mcconnell Taping in Subjects With Infrapatellar BursistisDocument4 pagesA Study On Effectiveness of Low Level Laser Therapy and Mcconnell Taping in Subjects With Infrapatellar BursistisInternational Journal of Innovative Science and Research TechnologyNo ratings yet
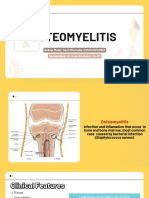
- OsteomyelitisDocument15 pagesOsteomyelitis2018B-04Desti RhomaliaNo ratings yet
- Pierre Robin Syndrome A Case ReportDocument2 pagesPierre Robin Syndrome A Case ReportResearch ParkNo ratings yet
- Basic of Ot 1Document2 pagesBasic of Ot 1shubham vermaNo ratings yet
- Isolated Third Nerve PalsyDocument4 pagesIsolated Third Nerve PalsySora KerovaNo ratings yet
- Peelings PDFDocument222 pagesPeelings PDFEdy Estévez100% (3)
- Moral and Ethical IssuesDocument16 pagesMoral and Ethical IssuesZunaira ArshadNo ratings yet
- Running Head: Music Therapy and Its Effect On Dementia 1: April 11, 2021Document7 pagesRunning Head: Music Therapy and Its Effect On Dementia 1: April 11, 2021api-641835925No ratings yet
- Euro Ophthalmology 2020 Scientific ProgramDocument7 pagesEuro Ophthalmology 2020 Scientific ProgramAnonymous izTmUWnNo ratings yet