You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Use of Folk Healing Medicines by Selected African-American WomenDocument191 pagesThe Use of Folk Healing Medicines by Selected African-American WomenPi-Ankhi Afuraka Kaneset100% (1)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Best Quotes of All Time.Document25 pagesBest Quotes of All Time.Abhi SharmaNo ratings yet
- ClonidineDocument1 pageClonidineRo-anne Aku50% (2)
- Atorvastatin CalciumDocument1 pageAtorvastatin CalciumRo-anne AkuNo ratings yet
- FIGO Accreta Prenantal DiagnosisDocument7 pagesFIGO Accreta Prenantal DiagnosisYosef Dwi Cahyadi SalanNo ratings yet
- Theories of human development and the thinkers behind themDocument4 pagesTheories of human development and the thinkers behind themRo-anne Aku100% (1)
- Abdominal Pain NCPDocument3 pagesAbdominal Pain NCPRo-anne Aku100% (1)
- TORCH in PregnancyDocument122 pagesTORCH in PregnancyroserosannaNo ratings yet
- PRC-BON Memorandum Order No. 2-b Series of 2009Document5 pagesPRC-BON Memorandum Order No. 2-b Series of 2009PhilippineNursingDirectory.com100% (3)
- Famtypo TallyDocument3 pagesFamtypo TallyRo-anne AkuNo ratings yet
- Form - Actual DeliveryDocument1 pageForm - Actual DeliveryRo-anne AkuNo ratings yet
- 1-15 16-26 27-40 I. Demographic Variables Family StructureDocument36 pages1-15 16-26 27-40 I. Demographic Variables Family StructureRo-anne AkuNo ratings yet
- Tally SheetDocument2 pagesTally SheetRo-anne AkuNo ratings yet
- Com Diag TallyDocument5 pagesCom Diag TallyRo-anne AkuNo ratings yet
- ZonisamideDocument2 pagesZonisamideRo-anne AkuNo ratings yet
- Com Diag TallyDocument5 pagesCom Diag TallyRo-anne AkuNo ratings yet
- The Life of Harvey: 1 Part: My AutobiographyDocument6 pagesThe Life of Harvey: 1 Part: My AutobiographyRo-anne AkuNo ratings yet
- Phospo-Soda Laxative Mechanism, Dosage, Side EffectsDocument1 pagePhospo-Soda Laxative Mechanism, Dosage, Side EffectsRo-anne AkuNo ratings yet
- Gelatin (Jelly Thin) 12 Cups Water With Pandan Leaves 3 Bars Gulaman 2 Cans Evaporated Milk 2 Cans Condensed Milk 1 KG Sugar PineappleDocument1 pageGelatin (Jelly Thin) 12 Cups Water With Pandan Leaves 3 Bars Gulaman 2 Cans Evaporated Milk 2 Cans Condensed Milk 1 KG Sugar PineappleRo-anne AkuNo ratings yet
- University of Perpetual Help SystemDocument1 pageUniversity of Perpetual Help SystemRo-anne AkuNo ratings yet
- Reduce Infection Risk for Patient with Weak DefensesDocument2 pagesReduce Infection Risk for Patient with Weak DefensesRo-anne AkuNo ratings yet
- Drug Action Indication Side Effect Adverse Effect Nursing ConsiderationsDocument1 pageDrug Action Indication Side Effect Adverse Effect Nursing ConsiderationsRo-anne AkuNo ratings yet
- Social Change 1Document1 pageSocial Change 1Ro-anne AkuNo ratings yet
- System InfoDocument1 pageSystem Infoailene_avila20108568No ratings yet
- System InfoDocument1 pageSystem Infoailene_avila20108568No ratings yet
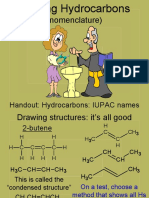
- (Nomenclature) : Handout: Hydrocarbons: IUPAC NamesDocument28 pages(Nomenclature) : Handout: Hydrocarbons: IUPAC NamesRo-anne AkuNo ratings yet
- Drug Action Indication Contraindication Side Effect Adverse Effect Nursing ConsiderationsDocument3 pagesDrug Action Indication Contraindication Side Effect Adverse Effect Nursing ConsiderationsRo-anne AkuNo ratings yet
- Post-Op Patient Infection Risk ManagementDocument1 pagePost-Op Patient Infection Risk ManagementRo-anne AkuNo ratings yet
- Risk For InjuryDocument2 pagesRisk For InjuryRo-anne AkuNo ratings yet
- Cues Nursing Diagnosis Scientific Reason Planning Nursing Intervention EvaluationDocument1 pageCues Nursing Diagnosis Scientific Reason Planning Nursing Intervention EvaluationRo-anne AkuNo ratings yet
- Drug Study FormDocument1 pageDrug Study FormRo-anne AkuNo ratings yet
- Social Change 1Document1 pageSocial Change 1Ro-anne AkuNo ratings yet
- Rapp Ginsburg - Enabling DisabilityDocument24 pagesRapp Ginsburg - Enabling DisabilityTom JousselinNo ratings yet
- Goal Common Measures To Ensure Family-Centered Maternal and Child Health Care PrinciplesDocument2 pagesGoal Common Measures To Ensure Family-Centered Maternal and Child Health Care PrinciplesKen AgustinNo ratings yet
- 2015 Article 110Document9 pages2015 Article 110Boleac HaralambieNo ratings yet
- Contraceptive Pill GuideDocument8 pagesContraceptive Pill GuideMr. CrustNo ratings yet
- Teenage Pregnancy in The PhilippinesDocument7 pagesTeenage Pregnancy in The PhilippinesJanine Marie CaprichosaNo ratings yet
- CHN Work GuideDocument2 pagesCHN Work GuideKeisha BartolataNo ratings yet
- Ingles Caderno de Provas e Chave de Respostas - Edital 07-2023Document8 pagesIngles Caderno de Provas e Chave de Respostas - Edital 07-2023Eduarda HelenaNo ratings yet
- Pil 3530 PDFDocument1 pagePil 3530 PDFAfief I-Fadha NxNo ratings yet
- Child Development A Cultural Approach 2nd Edition Arnett Solutions ManualDocument36 pagesChild Development A Cultural Approach 2nd Edition Arnett Solutions Manualunframecizarsidquu100% (21)
- CASE PRE (Intrapartum)Document6 pagesCASE PRE (Intrapartum)teuuuuNo ratings yet
- Recurrent MiscarriageDocument5 pagesRecurrent MiscarriagedindaNo ratings yet
- Feoutal AddDocument9 pagesFeoutal AddDHUPGURI DIAGNOSTICNo ratings yet
- Article 257. Unintentional Abortion ElementsDocument3 pagesArticle 257. Unintentional Abortion ElementsJason ToddNo ratings yet
- Data AnalysisDocument1 pageData AnalysisRicardoNo ratings yet
- Monitoring key dermatologic medicationsDocument3 pagesMonitoring key dermatologic medicationsriskhakovNo ratings yet
- Concept PaperDocument3 pagesConcept PaperJANELLE TAMSYNE MONTIVEROSNo ratings yet
- Test Bank For Financial Management Core Concepts 2nd Edition Raymond BrooksDocument34 pagesTest Bank For Financial Management Core Concepts 2nd Edition Raymond Brooksrowdydow.shittimu4n3100% (44)
- 8 Steps To A Healthy PregnancyDocument4 pages8 Steps To A Healthy Pregnancybeverly-cope-6067No ratings yet
- Post Abortion Care (Pac)Document9 pagesPost Abortion Care (Pac)Ekiran BabajideNo ratings yet
- Clinical Guideline: Sepsis in PregnancyDocument24 pagesClinical Guideline: Sepsis in PregnancyYerni DaeliNo ratings yet
- Problem in PregnancyDocument4 pagesProblem in PregnancyYumiSapta KanaNo ratings yet
- Prenatal weight gain chartDocument1 pagePrenatal weight gain chartmaKitten08No ratings yet
- Ethnographic Analysis of Savara Tribe in India: Delliswararao KonduruDocument14 pagesEthnographic Analysis of Savara Tribe in India: Delliswararao KonduruUmashankar VadrevuNo ratings yet
- Estimation of Degree of CalcinationDocument30 pagesEstimation of Degree of CalcinationRashmi100% (1)
- Common Fears Related To Pregnancy, Labor, and Delivery and Coping Mechanisms Among Primigravida MothersDocument70 pagesCommon Fears Related To Pregnancy, Labor, and Delivery and Coping Mechanisms Among Primigravida MothersSmile Tambanillo0% (1)
- Understanding Addiction's Impact on Individuals, Families & CommunitiesDocument4 pagesUnderstanding Addiction's Impact on Individuals, Families & CommunitiesUmm ZainabNo ratings yet
- Sample MCQ QuestionsDocument11 pagesSample MCQ QuestionsPreeti ChouhanNo ratings yet