You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Parthasarathy2013 PDFDocument7 pagesParthasarathy2013 PDFAndi BintangNo ratings yet
- Sacral Nerve Stimulation Reduces Elevated Urinary Nerve Growth Factor Levels in Women With Symptomatic Detrusor OveractivityDocument5 pagesSacral Nerve Stimulation Reduces Elevated Urinary Nerve Growth Factor Levels in Women With Symptomatic Detrusor OveractivityAndi BintangNo ratings yet
- Medical Hypotheses: Yixian Li, Juan Zhou, Ian Burkovskiy, Pollen Yeung, Christian Lehmann TDocument3 pagesMedical Hypotheses: Yixian Li, Juan Zhou, Ian Burkovskiy, Pollen Yeung, Christian Lehmann TAndi BintangNo ratings yet
- Subarachnoid Block For Caesarean Section in Severe PreeclampsiaDocument6 pagesSubarachnoid Block For Caesarean Section in Severe PreeclampsiaAndi BintangNo ratings yet
- 1 s2.0 S0002937800704534 Main PDFDocument1 page1 s2.0 S0002937800704534 Main PDFAndi BintangNo ratings yet
- Depresión e InmunidadDocument13 pagesDepresión e InmunidadgabisaenaNo ratings yet
- Bar A Zanchi 2018Document17 pagesBar A Zanchi 2018Andi BintangNo ratings yet
- Anestesia General para Césarea PDFDocument7 pagesAnestesia General para Césarea PDFAgnese ValentiniNo ratings yet
- Anestesia General para Césarea PDFDocument7 pagesAnestesia General para Césarea PDFAgnese ValentiniNo ratings yet
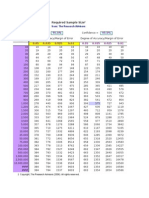
- Required Sample Size: From: The Research AdvisorsDocument3 pagesRequired Sample Size: From: The Research AdvisorsAbhishek Sharma100% (1)
- Procalcitonin As A Biomarker of Severity Degree in Sepsis Due To PneumoniaDocument5 pagesProcalcitonin As A Biomarker of Severity Degree in Sepsis Due To PneumoniaAndi BintangNo ratings yet
- 2013 Student Membership ApplicationDocument1 page2013 Student Membership ApplicationAndi BintangNo ratings yet
- Cultural Sociology of Mental Illness n28Document5 pagesCultural Sociology of Mental Illness n28Andi BintangNo ratings yet
- Overweight linked to increased risk of lower back painDocument8 pagesOverweight linked to increased risk of lower back painAndi BintangNo ratings yet
- Instruction For Author ClimactericDocument9 pagesInstruction For Author ClimactericAndi BintangNo ratings yet
- 1 s2.0 S1052305714000561 MainDocument6 pages1 s2.0 S1052305714000561 MainAndi BintangNo ratings yet
- 1 s2.0 S0021755713002003 MainDocument6 pages1 s2.0 S0021755713002003 MainAndi BintangNo ratings yet
- Association Between Constipation and Colorectal Cancer Systematic Review and Meta-Analysis of Observational StusdgdiesDocument10 pagesAssociation Between Constipation and Colorectal Cancer Systematic Review and Meta-Analysis of Observational StusdgdiesAndi BintangNo ratings yet
- Hepatitis C APASLfghDocument27 pagesHepatitis C APASLfghAndi BintangNo ratings yet
- 1 s2.0 S0021755713002003 MainDocument6 pages1 s2.0 S0021755713002003 MainAndi BintangNo ratings yet
- 1 s2.0 S0002937803001388 MainDocument3 pages1 s2.0 S0002937803001388 MainAndi BintangNo ratings yet
- Prevalence of Diabetes and Impaired Fasting Glucose in Adults in The U.S. PopulationDocument6 pagesPrevalence of Diabetes and Impaired Fasting Glucose in Adults in The U.S. PopulationAndi BintangNo ratings yet
- Anthropometry: Ergonomics Additional ResourcesDocument5 pagesAnthropometry: Ergonomics Additional ResourcesAndi BintangNo ratings yet
- Urologi PDFDocument237 pagesUrologi PDFAndi BintangNo ratings yet
- Serviks DocjhjuDocument366 pagesServiks DocjhjuAndi BintangNo ratings yet
- MK Giz Slide Infant Feeding PracticeDocument1 pageMK Giz Slide Infant Feeding PracticeAndi BintangNo ratings yet
- PCT CAP ABiuytoDocument10 pagesPCT CAP ABiuytoAndi BintangNo ratings yet
- Cap Bts 2009 ComplitdgDocument139 pagesCap Bts 2009 ComplitdgAndi BintangNo ratings yet
- ATS Guidelines CAP ManagementDocument25 pagesATS Guidelines CAP ManagementMae Matira AbeladorNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- People Vs MadridDocument5 pagesPeople Vs MadridEunice SerneoNo ratings yet
- People v. EnriquezDocument2 pagesPeople v. EnriquezChris Erwin AlquizalasNo ratings yet
- Stradec v. SidcDocument2 pagesStradec v. SidcFrancis Jan Ax ValerioNo ratings yet
- Palaganas Vs PalaganasDocument3 pagesPalaganas Vs PalaganasLucas Gabriel JohnsonNo ratings yet
- SampleDocument64 pagesSampleJunliegh permisonNo ratings yet
- FIFA World Cup Milestones, Facts & FiguresDocument25 pagesFIFA World Cup Milestones, Facts & FiguresAleks VNo ratings yet
- Boulder District Attorneys Office Letter To Kathleen ChippiDocument1 pageBoulder District Attorneys Office Letter To Kathleen ChippiMichael_Lee_RobertsNo ratings yet
- Suffer in Silence A Novel of Navy SEAL TrainingDocument13 pagesSuffer in Silence A Novel of Navy SEAL TrainingMacmillan Publishers100% (1)
- Check Encumberance Certificate To Verify Property TitleDocument2 pagesCheck Encumberance Certificate To Verify Property TitlePVV RAMA RAONo ratings yet
- Dumaual - Crim Rev DigestsDocument18 pagesDumaual - Crim Rev DigestsJanjan DumaualNo ratings yet
- Forensic Examination Report - Kevin SplittgerberDocument16 pagesForensic Examination Report - Kevin Splittgerberapi-546415174No ratings yet
- IHL 1 BALLB ProjectDocument16 pagesIHL 1 BALLB Projectabcde fghikjNo ratings yet
- Research Proposal Sex Addiction FinalDocument14 pagesResearch Proposal Sex Addiction Finalapi-296203840100% (1)
- SCOUT OATH EXPLAINEDDocument8 pagesSCOUT OATH EXPLAINEDpiperNo ratings yet
- Strategies for Ending the Sino-Japanese and Russo-Japanese WarsDocument18 pagesStrategies for Ending the Sino-Japanese and Russo-Japanese Warscoca COLANo ratings yet
- MODULE 5 - Rizal PDFDocument12 pagesMODULE 5 - Rizal PDFKyle CuiNo ratings yet
- Supreme Court upholds dismissal of worker for serious misconductDocument2 pagesSupreme Court upholds dismissal of worker for serious misconductJoseNo ratings yet
- Esseye Medhin - 2002 - Addis Ababa Art Scene RevisitedDocument10 pagesEsseye Medhin - 2002 - Addis Ababa Art Scene RevisitedBirukyeNo ratings yet
- Sy Vs Judge DinopolDocument2 pagesSy Vs Judge DinopolMarianne Domingo100% (1)
- Judicial Clemency GuidelinesDocument13 pagesJudicial Clemency GuidelinesMunchie MichieNo ratings yet
- Special Marriage Act provisions for interfaith unionsDocument28 pagesSpecial Marriage Act provisions for interfaith unionsVed AntNo ratings yet
- Valencia V CADocument10 pagesValencia V CApjNo ratings yet
- People v Rafael Conviction Upheld for Frustrated Murder and MurderDocument35 pagesPeople v Rafael Conviction Upheld for Frustrated Murder and MurderNigel AlinsugNo ratings yet
- Boarding PassDocument2 pagesBoarding PassRupèsh GundechäNo ratings yet
- Municipal Ordinance No. 2015-01: Office of The Sangguniang BayanDocument4 pagesMunicipal Ordinance No. 2015-01: Office of The Sangguniang BayanEden Celestino Sarabia CachoNo ratings yet
- Geodesign BH Sos BrasilandiaDocument22 pagesGeodesign BH Sos BrasilandiaAdriana SandreNo ratings yet
- Resolution For AppointmentDocument3 pagesResolution For Appointmentjerome geoligaoNo ratings yet
- Status of Children in Conflict With The Law in La Trinidad 1325749101Document6 pagesStatus of Children in Conflict With The Law in La Trinidad 1325749101Jan Igor GalinatoNo ratings yet
- Ship Stability Notes BS222Document74 pagesShip Stability Notes BS222Ahmed Aboelmagd100% (1)
- Freedom of Information ActsDocument22 pagesFreedom of Information ActsSarah_GadNo ratings yet