You might also like
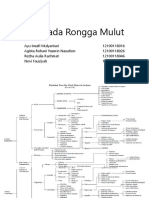
- Lesi pada Rongga MulutDocument70 pagesLesi pada Rongga MulutAyu InsafiNo ratings yet
- AchantosisDocument2 pagesAchantosisAyu InsafiNo ratings yet
- Cerebral Palsy: Anatomi, Etiologi, Manifestasi Klinik dan DiagnosisDocument12 pagesCerebral Palsy: Anatomi, Etiologi, Manifestasi Klinik dan DiagnosisAyu InsafiNo ratings yet
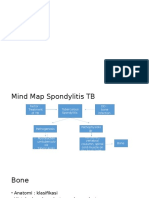
- SpondylosisDocument15 pagesSpondylosisAyu InsafiNo ratings yet
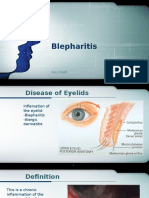
- Blepharitis: Inflammation of the EyelidsDocument17 pagesBlepharitis: Inflammation of the EyelidsAyu InsafiNo ratings yet
- PSM Unpad Env and Musculosclt EmergenciesDocument27 pagesPSM Unpad Env and Musculosclt EmergenciesAyu InsafiNo ratings yet
- Abstract Mental Health Status Among Preschooler Children With Gadget Use HabitualDocument1 pageAbstract Mental Health Status Among Preschooler Children With Gadget Use HabitualAyu InsafiNo ratings yet
- Blepharitis: Inflammation of the EyelidsDocument17 pagesBlepharitis: Inflammation of the EyelidsAyu InsafiNo ratings yet
- Abstract Mental Health Status Among Preschooler Children With Gadget Use HabitualDocument1 pageAbstract Mental Health Status Among Preschooler Children With Gadget Use HabitualAyu InsafiNo ratings yet
- THYROID PHYSIOLOGY AND DEVELOPMENT: HORMONES, SCREENING, TREATMENTDocument1 pageTHYROID PHYSIOLOGY AND DEVELOPMENT: HORMONES, SCREENING, TREATMENTAyu InsafiNo ratings yet
- How tumors develop blood vessels through angiogenesisDocument2 pagesHow tumors develop blood vessels through angiogenesisAyu InsafiNo ratings yet
- Physchiatric DisorderDocument1 pagePhyschiatric DisorderAyu InsafiNo ratings yet
- Co IntoxicationDocument31 pagesCo IntoxicationAyu InsafiNo ratings yet
- Genetics of Human Neural Tube DefectsDocument7 pagesGenetics of Human Neural Tube DefectsAyu InsafiNo ratings yet
- Physchiatric DisorderDocument1 pagePhyschiatric DisorderAyu InsafiNo ratings yet
- Ten Step To Successful Breeastfeeding Is An Goverment Attempt To Increase The ExclusiveDocument1 pageTen Step To Successful Breeastfeeding Is An Goverment Attempt To Increase The ExclusiveAyu InsafiNo ratings yet
- Stroke PlenoDocument30 pagesStroke PlenoAyu InsafiNo ratings yet
- PatmekDocument1 pagePatmekAyu InsafiNo ratings yet
- How To Wash Your HandsDocument13 pagesHow To Wash Your HandsAyu InsafiNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Types of Addictions: How We Treat Them: Alcohol AddictionDocument4 pagesTypes of Addictions: How We Treat Them: Alcohol AddictionJubelee Anne PatanganNo ratings yet
- Sena, Zyrus Reoder ADocument4 pagesSena, Zyrus Reoder AAkoSiIngridNo ratings yet
- Research in Autism Spectrum Disorders: Anika Langmann, Joachim Becker, Luise Poustka, Katja Becker, Inge Kamp-BeckerDocument10 pagesResearch in Autism Spectrum Disorders: Anika Langmann, Joachim Becker, Luise Poustka, Katja Becker, Inge Kamp-BeckerVictor NamurNo ratings yet
- Case Report: SymptomsDocument4 pagesCase Report: Symptomsapi-339983807No ratings yet
- OCPD FinalDocument9 pagesOCPD FinalAna16ANo ratings yet
- Battering Typologies, Attachment Insecurity, and Personality Disorders-A Comprehensive Literature ReviewDocument18 pagesBattering Typologies, Attachment Insecurity, and Personality Disorders-A Comprehensive Literature Reviewjulian gomez sosaNo ratings yet
- Adhd Presentation 1Document8 pagesAdhd Presentation 1api-314230015No ratings yet
- Somatizare ChestionarDocument9 pagesSomatizare ChestionaralinaGHERGHISANNo ratings yet
- Psychiatric NursingDocument12 pagesPsychiatric NursingLloyd Rafael Estabillo100% (1)
- Parent NewsletterDocument4 pagesParent Newsletterapi-301094873No ratings yet
- Psychiatry Dr. Osama Mahmoud PDFDocument59 pagesPsychiatry Dr. Osama Mahmoud PDFRaouf Ra'fat SolimanNo ratings yet
- 01 Psychiatric Assessment & DSM-5 BBDocument62 pages01 Psychiatric Assessment & DSM-5 BBDhillonvNo ratings yet
- PTSD Criteria DSM 5Document2 pagesPTSD Criteria DSM 5Liv MNo ratings yet
- The 3D Quiz: Review The Handout "3Ds", Then Answer The Following QuestionsDocument4 pagesThe 3D Quiz: Review The Handout "3Ds", Then Answer The Following Questionsvladimirkulf2142No ratings yet
- Health Education Substance AbuseDocument13 pagesHealth Education Substance Abusekiran mahal100% (2)
- ATPDDocument11 pagesATPDsagar189No ratings yet
- Case Vignette Assignment 3Document2 pagesCase Vignette Assignment 3mysteryvan19810% (1)
- NEW RESEARCH AntipshychoticDocument319 pagesNEW RESEARCH AntipshychoticLaura BechtolsheimerNo ratings yet
- Bipolar Disorder: Joseph Jakeem Lozada - Grade 12 DeuteronomyDocument2 pagesBipolar Disorder: Joseph Jakeem Lozada - Grade 12 DeuteronomyJJ LozadaNo ratings yet
- Bulgarian PsychiatryDocument12 pagesBulgarian PsychiatrykarlunchoNo ratings yet
- Mindfulness-Based Cognitive Therapy For Depression, PDFDocument73 pagesMindfulness-Based Cognitive Therapy For Depression, PDFFRosariopsi50% (2)
- Affective DisorderDocument25 pagesAffective DisordermengakuNo ratings yet
- FASD Summer CampsDocument2 pagesFASD Summer CampsfasdunitedNo ratings yet
- Mood Disorders - Lecture NotesDocument24 pagesMood Disorders - Lecture NotesPeter Forster100% (9)
- Initial EvaluationDocument2 pagesInitial EvaluationStephan CarlsonNo ratings yet
- Berman (1995)Document14 pagesBerman (1995)stupidshitNo ratings yet
- Understanding Psychosis and SchizophreniaDocument32 pagesUnderstanding Psychosis and SchizophreniaAnonymous zxTFUoqzklNo ratings yet
- Common Emotional and Behavioral Disorders in PreschoolersDocument25 pagesCommon Emotional and Behavioral Disorders in PreschoolersAlkistis MarinakiNo ratings yet
- Kleptomania and HomoeopathyDocument7 pagesKleptomania and HomoeopathyDr. Rajneesh Kumar Sharma MD HomNo ratings yet
- Anorexia PaperDocument6 pagesAnorexia Paperapi-254016016No ratings yet