You might also like
- 2011 Spring SOCCER Registration FormDocument3 pages2011 Spring SOCCER Registration FormalabastercityhNo ratings yet
- 2011 Spring BASEBALL Registration FormDocument2 pages2011 Spring BASEBALL Registration FormalabastercityhNo ratings yet
- Af Cavemen Cheer Try-Out PacketDocument5 pagesAf Cavemen Cheer Try-Out PacketAf CheerNo ratings yet
- 2011 Spring Soccer Registration Form 1-28-11Document1 page2011 Spring Soccer Registration Form 1-28-11jmercier74No ratings yet
- Key-Club-Membership-Form 1Document4 pagesKey-Club-Membership-Form 1api-461627977No ratings yet
- TEMPLATE Medical Release WITHOUT Notary 1Document1 pageTEMPLATE Medical Release WITHOUT Notary 1Peter WagnerNo ratings yet
- SummersportsDocument1 pageSummersportsapi-318790212No ratings yet
- Camp Jeff Waiver Form - 2021Document2 pagesCamp Jeff Waiver Form - 2021Nolan HahnNo ratings yet
- 2013-2014 Returning Medical FormDocument10 pages2013-2014 Returning Medical FormKevin WangNo ratings yet
- Genesis Academy Pre-K Program Registration Form: Child's InformationDocument7 pagesGenesis Academy Pre-K Program Registration Form: Child's InformationPhillip M JonesNo ratings yet
- JR High 2010 Registration FormDocument4 pagesJR High 2010 Registration FormryanlashleeNo ratings yet
- Allen County Board of DD Student Emergency DataDocument2 pagesAllen County Board of DD Student Emergency Dataadhi eng lrtNo ratings yet
- Fall 2011 RecRegistrationFormDocument1 pageFall 2011 RecRegistrationFormnikkistoneNo ratings yet
- Club Membership FormDocument2 pagesClub Membership Formapi-253006949No ratings yet
- Accepted. Please Send The Completed Forms ToDocument18 pagesAccepted. Please Send The Completed Forms ToAmber Schmidt DoopNo ratings yet
- SV GLORY Medical Release-Emergency Form & Liability Waiver FormDocument2 pagesSV GLORY Medical Release-Emergency Form & Liability Waiver FormfcuevasNo ratings yet
- Teen MedicalDocument1 pageTeen MedicalJohn C StarkNo ratings yet
- Inter College Team Sports Basketball Volleyball MechanicsDocument2 pagesInter College Team Sports Basketball Volleyball MechanicsZhennaica Coreen NavarroNo ratings yet
- MGT Waiver FormDocument1 pageMGT Waiver Formjtmott00No ratings yet
- Greater Houston Area Chapter American Red Cross Youth Volunteer Application FormDocument6 pagesGreater Houston Area Chapter American Red Cross Youth Volunteer Application FormLauren KhooNo ratings yet
- Liability and Consent FormDocument2 pagesLiability and Consent Formapi-19917129No ratings yet
- EUREKA HIGH SOFTBALL Clinic Participant InfoDocument1 pageEUREKA HIGH SOFTBALL Clinic Participant InfoSandra MendozaNo ratings yet
- Official Medical Information and Release FormDocument2 pagesOfficial Medical Information and Release FormtheNOLAtreeNo ratings yet
- Parental Consent Work Immersion 2022Document1 pageParental Consent Work Immersion 2022Mark Lorenz BaranganNo ratings yet
- Studentnotice 1349953350Document4 pagesStudentnotice 1349953350AadityaNo ratings yet
- Go BIG For Parkinson Registration FormDocument2 pagesGo BIG For Parkinson Registration Formrickberry55No ratings yet
- Pds Medical-Cert Waiver 2023-RspcDocument1 pagePds Medical-Cert Waiver 2023-RspcRon MenesNo ratings yet
- Registration Form May 23Document9 pagesRegistration Form May 23Krishn PatelNo ratings yet
- Return Completed (Both Sides) Registration Form With CheckDocument2 pagesReturn Completed (Both Sides) Registration Form With CheckFrancis HerouxNo ratings yet
- Field Trip Permission Slip FillableDocument1 pageField Trip Permission Slip Fillabletvtcf286v9No ratings yet
- Paintball Release 2008Document1 pagePaintball Release 2008jackcharNo ratings yet
- Parks Program - Registration 2011Document5 pagesParks Program - Registration 2011rob_crowell_1No ratings yet
- Adventurer Club Registration Health RecordDocument2 pagesAdventurer Club Registration Health RecordJosie MocevakacaNo ratings yet
- Medical Release FormDocument1 pageMedical Release FormNicole LeongNo ratings yet
- 4.2022 SCSC Membership FormDocument2 pages4.2022 SCSC Membership FormLerbet SisonNo ratings yet
- Group Real Registration Form 1 - 3Document3 pagesGroup Real Registration Form 1 - 3api-259107792No ratings yet
- Medical Release FormDocument1 pageMedical Release Formkelschriver12No ratings yet
- Club Application 2011Document1 pageClub Application 2011mccorvey111No ratings yet
- Parent Consent Form For MembershipDocument1 pageParent Consent Form For MembershipFern RoseNo ratings yet
- Student Profile Form For Inventory - PDFDocument2 pagesStudent Profile Form For Inventory - PDFLeen Ganoran100% (1)
- Apply for Co-op MembershipDocument1 pageApply for Co-op MembershipReshel BulcaseNo ratings yet
- Register Now for DeKalb County Summer CampDocument2 pagesRegister Now for DeKalb County Summer CampDennis HendNo ratings yet
- Velocity Health FormDocument2 pagesVelocity Health FormChris HansenNo ratings yet
- Out Front Theatre Summer FormDocument2 pagesOut Front Theatre Summer FormJacobNo ratings yet
- New Enrolment Form SDJDDocument9 pagesNew Enrolment Form SDJDsurendra mohapatraNo ratings yet
- Writable PC FormDocument1 pageWritable PC FormJulie Vyne ModalesNo ratings yet
- Revolution Lock inDocument1 pageRevolution Lock inkjbennett56No ratings yet
- City Meet 2023 Parental Consent FormDocument1 pageCity Meet 2023 Parental Consent FormJERUSALEM DE GUZMANNo ratings yet
- PDS Medical RSPCDocument1 pagePDS Medical RSPCMyka Andrea GarciaNo ratings yet
- HRD Form 001 Employee Application Gen - Admin v.001Document3 pagesHRD Form 001 Employee Application Gen - Admin v.001DadangNo ratings yet
- RKC Reg FormDocument10 pagesRKC Reg FormkalpitNo ratings yet
- Admission Form 2008Document2 pagesAdmission Form 2008Abbas AliNo ratings yet
- 2014 SJCSC SJCYFL Registration Form (Junior, Major & Senior) - Final PDFDocument2 pages2014 SJCSC SJCYFL Registration Form (Junior, Major & Senior) - Final PDFBen A AriffinNo ratings yet
- SWORN STATEMENT OF ACTUAL CARE AND CUSTODY RevisedDocument1 pageSWORN STATEMENT OF ACTUAL CARE AND CUSTODY Revisedkenjiecastillo433No ratings yet
- Core Team 22-23 RegistrationDocument8 pagesCore Team 22-23 Registrationjakertomay7No ratings yet
- My Sam Ember Ship FormDocument1 pageMy Sam Ember Ship FormpiratedadNo ratings yet
- Parental Consent and Waiver Form For MinorsDocument1 pageParental Consent and Waiver Form For MinorsTiffany BabyNo ratings yet
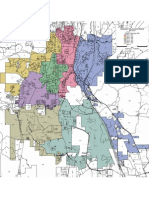
- 2012 Alabaster Ward MapDocument1 page2012 Alabaster Ward Mapalabastercityh0% (2)
- Alabaster Newsletter Dec 10Document32 pagesAlabaster Newsletter Dec 10alabastercityhNo ratings yet
- Alabaster Ward Map 2008 PDFDocument1 pageAlabaster Ward Map 2008 PDFalabastercityhNo ratings yet
- Alabaster Newsletter Feb 2011Document32 pagesAlabaster Newsletter Feb 2011alabastercityhNo ratings yet
- 2011 Spring Girl's SOFTBALL Registration FormDocument2 pages2011 Spring Girl's SOFTBALL Registration FormalabastercityhNo ratings yet
- 10 BV PDFDocument13 pages10 BV PDFYossy VesriNo ratings yet
- Aeromedical Transport TPDocument8 pagesAeromedical Transport TPgalib20No ratings yet
- Nuclear Associates User ManualDocument20 pagesNuclear Associates User ManualvandarsNo ratings yet
- ACHALASIADocument31 pagesACHALASIAkhan jeetNo ratings yet
- Aman Foundation Internship Application FormDocument4 pagesAman Foundation Internship Application Formabdullahnisar92No ratings yet
- MSDS+Styrene+From+Sigma AldrichDocument7 pagesMSDS+Styrene+From+Sigma AldrichYaumi IstiqlaliyahNo ratings yet
- Herb II-5-Herbs That Tonify Qi & BloodDocument51 pagesHerb II-5-Herbs That Tonify Qi & BloodEdison halimNo ratings yet
- What Is HumorDocument5 pagesWhat Is HumorWan Sek ChoonNo ratings yet
- Boyd Et Al-2019-Cochrane Database of Systematic ReviewsDocument38 pagesBoyd Et Al-2019-Cochrane Database of Systematic ReviewsomyNo ratings yet
- Unipex - Technical - Exo-PDocument6 pagesUnipex - Technical - Exo-PFelpnilNo ratings yet
- Semen AnalysisDocument2 pagesSemen AnalysisSabir KamalNo ratings yet
- 0100 Sigmazam ReducerDocument2 pages0100 Sigmazam ReducerAhmed SaadNo ratings yet
- Ethnomedicinal Survey Report On Plants of Tribal Regions of Anuppur 270Document3 pagesEthnomedicinal Survey Report On Plants of Tribal Regions of Anuppur 270Medtext PublicationsNo ratings yet
- Pathology of JointsDocument13 pagesPathology of JointswobblegobbleNo ratings yet
- Wiki Apgar Score01Document3 pagesWiki Apgar Score01Leevon ThomasNo ratings yet
- Ee Mock Test 2 Jan 2017 Qa 2Document92 pagesEe Mock Test 2 Jan 2017 Qa 2EmadSamirNo ratings yet
- 10 Furunculosis (Aeromonas Salmonicida)Document86 pages10 Furunculosis (Aeromonas Salmonicida)Jose AntonioNo ratings yet
- HTC Intake Form - September 4 - Final - Doc 7.9.13Document10 pagesHTC Intake Form - September 4 - Final - Doc 7.9.13Kealeboga Duece ThoboloNo ratings yet
- NCP CompilationDocument11 pagesNCP CompilationRene John FranciscoNo ratings yet
- Pink Panther - Diabetes Management - Chapter 9Document16 pagesPink Panther - Diabetes Management - Chapter 9jennmoyerNo ratings yet
- Maximum Marks: 100Document35 pagesMaximum Marks: 100Yu HoyanNo ratings yet
- 3 Azarpour Et Al. JNBR 4 (1) 2015 PDFDocument9 pages3 Azarpour Et Al. JNBR 4 (1) 2015 PDFKamailNo ratings yet
- Reasoning BookDocument38 pagesReasoning BookAshish Sharma100% (1)
- Abdominal Aortic AneurysmDocument20 pagesAbdominal Aortic AneurysmPortia Rose RodriguezNo ratings yet
- Not Eligible As No Experience of Teaching and ResearchDocument5 pagesNot Eligible As No Experience of Teaching and ResearchVasanth Kumar AllaNo ratings yet
- Types of Casts and Their IndicationsDocument3 pagesTypes of Casts and Their IndicationsPhylum ChordataNo ratings yet
- Cir 0000000000000899Document25 pagesCir 0000000000000899hanifa ambNo ratings yet
- Advances in Psychological and Social Support After DisastersDocument149 pagesAdvances in Psychological and Social Support After DisastersjprewittdiazNo ratings yet
- ECG Identification QuizDocument40 pagesECG Identification QuizRahul AudenesenNo ratings yet
- Forever ARGI+® Stick Packet Product InformationDocument1 pageForever ARGI+® Stick Packet Product InformationArif Zaman SiddiqueNo ratings yet