You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Shoulder ExaminationDocument2 pagesShoulder ExaminationabhandlungNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Cardiac AuscultationDocument7 pagesCardiac AuscultationabhandlungNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Examination in NeonatesDocument7 pagesExamination in Neonatesabhandlung100% (6)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Esophageal CancerDocument23 pagesEsophageal Cancerabhandlung100% (3)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Rashes Can Be Described AsDocument4 pagesRashes Can Be Described AsabhandlungNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Management of Severe Hypertension, Hypertension in Special ConditionDocument43 pagesManagement of Severe Hypertension, Hypertension in Special Conditionabhandlung100% (3)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Examination in PregnancyDocument3 pagesExamination in Pregnancyabhandlung100% (5)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Pocket Guide For Asthma Management and PreventionDocument30 pagesPocket Guide For Asthma Management and PreventionRizalNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Chronic Suppurative Otitis MediaDocument11 pagesChronic Suppurative Otitis Mediaabhandlung100% (1)
- Chapter 7 - NERVOUS SYSTEM PDFDocument58 pagesChapter 7 - NERVOUS SYSTEM PDFMary LimlinganNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
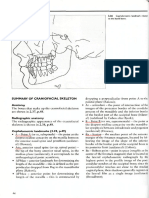
- Puntos CefalometricosDocument3 pagesPuntos Cefalometricosdg19060374No ratings yet
- The Basic Forms: A Sphere As The CraniumDocument5 pagesThe Basic Forms: A Sphere As The CraniumRaj RoyNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A To Z Orthodontics. Volume 22: History Taking and ExaminationDocument39 pagesA To Z Orthodontics. Volume 22: History Taking and ExaminationDrRohan DasNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- AHIST Biomedical Sciences ENT Exam QuestionsDocument8 pagesAHIST Biomedical Sciences ENT Exam Questionsyvette kinyuyNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- CongenitalDocument18 pagesCongenitalMatheus EmmanuelNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Ventricles, Meninges and CSF: Prepared By: Dr. Shilan H. Karim Assistant Professor of Anatomy & HistologyDocument65 pagesVentricles, Meninges and CSF: Prepared By: Dr. Shilan H. Karim Assistant Professor of Anatomy & Histologylazo daraNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Nervous System (STD 9) Lesson Plan - Zeenat GaziDocument4 pagesNervous System (STD 9) Lesson Plan - Zeenat GaziZest SpiritNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- Pose Training The Areas Around Your Eyes and MouthDocument11 pagesPose Training The Areas Around Your Eyes and MouthJeevan Vajha100% (1)
- Cranial Nerve Examination OSCE GuideDocument26 pagesCranial Nerve Examination OSCE GuideAbdullah Basheer AL-AnaziNo ratings yet
- HP Thyroid Meds Conversion ChartDocument3 pagesHP Thyroid Meds Conversion ChartJeanNo ratings yet
- Special SenseDocument5 pagesSpecial SenseJeannie OgangNo ratings yet
- ENT Ear I Scenarios (Compiled)Document35 pagesENT Ear I Scenarios (Compiled)rumman tariqNo ratings yet
- Interaction Between Otorhinolaryngology and Orthodontics - Correlation Between The Nasopharyngeal Airway and The Craniofacial ComplexDocument8 pagesInteraction Between Otorhinolaryngology and Orthodontics - Correlation Between The Nasopharyngeal Airway and The Craniofacial ComplexGarciaNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Facial Nerve Paralysis ... NyangwidaDocument20 pagesFacial Nerve Paralysis ... NyangwidaSerowe MangaidaNo ratings yet
- Practical Application of Anatomy For The Dental Implant SurgeonDocument15 pagesPractical Application of Anatomy For The Dental Implant SurgeonSebastián BernalNo ratings yet
- FETAL SKULL PPT by Komal UpretiDocument24 pagesFETAL SKULL PPT by Komal UpretiKomal UpretiNo ratings yet
- Ll6mn Temporal Bone CT and MRI Anatomy A Guide To 3D Volumetric AcquisitionsDocument220 pagesLl6mn Temporal Bone CT and MRI Anatomy A Guide To 3D Volumetric AcquisitionsPJ Sandhu100% (1)
- MCQsDocument14 pagesMCQsapi-372634688% (8)
- Thyroglossal Duct Remnants-1Document7 pagesThyroglossal Duct Remnants-1Olivia -No ratings yet
- Daftar Pustaka DaniDocument3 pagesDaftar Pustaka Danidokter linggauNo ratings yet
- Development of - PPTX Maxilla NewDocument69 pagesDevelopment of - PPTX Maxilla Newshivadev100% (1)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Chapter - 2 THE NERVOUS SYSTEM NOTESDocument3 pagesChapter - 2 THE NERVOUS SYSTEM NOTESShri ShriNo ratings yet
- Traumatic Tympanic PerforationDocument14 pagesTraumatic Tympanic PerforationNatalia CvNo ratings yet
- The Neural Basis of Religious Cognition: Jordan Grafman, Irene Cristofori, Wanting Zhong, and Joseph BulbuliaDocument8 pagesThe Neural Basis of Religious Cognition: Jordan Grafman, Irene Cristofori, Wanting Zhong, and Joseph Bulbuliagion.nand100% (1)
- Sheena The EyeDocument9 pagesSheena The EyeSheena Yen de Pano-PagdalianNo ratings yet
- 19.sinonasal TumorsDocument246 pages19.sinonasal Tumorsfabian hernandez medinaNo ratings yet
- Fapc Finals.Document391 pagesFapc Finals.C BajamondeNo ratings yet
- Brain Implants: Presented by Neseka.S 19BMR048Document17 pagesBrain Implants: Presented by Neseka.S 19BMR04819BMR048 Neseka SNo ratings yet
- Norma BasalisDocument10 pagesNorma BasalisArshad hussainNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)