You might also like
- Luiza's CasesDocument123 pagesLuiza's CasesLeila CarvalhalNo ratings yet
- Imaging Techniques in Obstetrics: UltrasoundDocument8 pagesImaging Techniques in Obstetrics: UltrasoundAmmar AlnajjarNo ratings yet
- Ultrasound Scanning of Fetal AnomalyDocument19 pagesUltrasound Scanning of Fetal AnomalyFA Khan0% (1)
- Risk Factors for High-Risk PregnanciesDocument8 pagesRisk Factors for High-Risk PregnanciesLRDR UCMEDNo ratings yet
- Screening of High-Risk Pregnancy, Newer Modalities of DiagnosisDocument12 pagesScreening of High-Risk Pregnancy, Newer Modalities of DiagnosisSanthosh.S.U100% (8)
- USG Trimester 1 21-11-05Document78 pagesUSG Trimester 1 21-11-05nurmalidaseptiaNo ratings yet
- First Trimester Pregnancy & ComplicationsDocument5 pagesFirst Trimester Pregnancy & ComplicationsDrPranav SharmaNo ratings yet
- Final Ob ChecklistDocument21 pagesFinal Ob ChecklistAlbino Fulgencio Santos III100% (1)
- v13 p74 EthicalDocument7 pagesv13 p74 EthicalVincent FloraNo ratings yet
- Pelvic ExaminationDocument3 pagesPelvic ExaminationAdisorn ChaikitNo ratings yet
- MRKH DissertationDocument4 pagesMRKH DissertationWriteMyPaperForCheapUK100% (1)
- Prune Belly SyndromeDocument39 pagesPrune Belly SyndromeHudaNo ratings yet
- Prenatal Diagnosis Estimation of Foetal Age 1Document33 pagesPrenatal Diagnosis Estimation of Foetal Age 1Riya SinghNo ratings yet
- PLACENTA PREVIA TOTALIS CaseDocument19 pagesPLACENTA PREVIA TOTALIS CasebobtagubaNo ratings yet
- Biochemical Methods ObgDocument25 pagesBiochemical Methods ObgRupali AroraNo ratings yet
- Obstetrics and Gynecology Clerkship OverviewDocument16 pagesObstetrics and Gynecology Clerkship Overviewselvie8750% (2)
- Best Dr. Ronald DavidDocument7 pagesBest Dr. Ronald Davidhar shishNo ratings yet
- 03-First Trimester UsgDocument103 pages03-First Trimester UsgBharti Pant GahtoriNo ratings yet
- Understanding AmniocentesisDocument3 pagesUnderstanding AmniocentesisRavindraNo ratings yet
- Prenatal Diagnosis Methods and GoalsDocument22 pagesPrenatal Diagnosis Methods and GoalshusshamNo ratings yet
- Chen, WW SurgDocument4 pagesChen, WW SurgMichael ChenNo ratings yet
- Maternal and Fetal Wellbeing AssessmentDocument46 pagesMaternal and Fetal Wellbeing AssessmentmariaNo ratings yet
- VentrikulomegaliDocument2 pagesVentrikulomegaliAida NurwidyaNo ratings yet
- Abdominal Wall Defects Exomphalos (Omphalocele)Document5 pagesAbdominal Wall Defects Exomphalos (Omphalocele)Ahmad Ulil AlbabNo ratings yet
- Amniocentesis QF PCR and Array CGH Tests 2830 PILDocument4 pagesAmniocentesis QF PCR and Array CGH Tests 2830 PILlicencaNo ratings yet
- CVS Procedure ExplainedDocument5 pagesCVS Procedure ExplainedpriyankaNo ratings yet
- Ipcon Correctable Anomalies Panel - PPDocument95 pagesIpcon Correctable Anomalies Panel - PPDr Ankur BiswasNo ratings yet
- Ultrasound-Why, When, What Is FoundDocument15 pagesUltrasound-Why, When, What Is FoundDyAnna Williams GordonNo ratings yet
- Undescended Testicles, Retractile Testicles, and Testicular TorsionDocument7 pagesUndescended Testicles, Retractile Testicles, and Testicular TorsionYudhistira SuryamanggalaNo ratings yet
- Prenatal DiagnosisDocument26 pagesPrenatal DiagnosisShandy Suwanto PutraNo ratings yet
- Problem Description Clinical Findings Management: HydrocoeleDocument4 pagesProblem Description Clinical Findings Management: HydrocoeleKARAKTERNo ratings yet
- Dysfunction of The Genito-Urinary Tract: Dejene Edosa (BSC, MSC in CMW) July 2021Document25 pagesDysfunction of The Genito-Urinary Tract: Dejene Edosa (BSC, MSC in CMW) July 2021michaelNo ratings yet
- Pediatric and Adolescent Gynecologic Emergencies 2022Document16 pagesPediatric and Adolescent Gynecologic Emergencies 2022Felipe MayorcaNo ratings yet
- FMcase 1Document24 pagesFMcase 1Ryan Townsend100% (2)
- IUGRDocument8 pagesIUGRPat BuotNo ratings yet
- Screening and Diagnosis of High-Risk PregnancyDocument44 pagesScreening and Diagnosis of High-Risk PregnancyKavipriyaNo ratings yet
- Case Report Jai 3Document8 pagesCase Report Jai 3EACMed Nursing Station 5th FloorNo ratings yet
- Obstetric ExaminationDocument4 pagesObstetric ExaminationSusan GeorgeNo ratings yet
- 64-Year-Old With Postmenopausal BleedingDocument3 pages64-Year-Old With Postmenopausal BleedingMorita TakaNo ratings yet
- Ob Ati StudyDocument22 pagesOb Ati Studylpirman0580% (5)
- Ultrasound Diagnosis of Early Pregnancy LossDocument18 pagesUltrasound Diagnosis of Early Pregnancy LossxxdrivexxNo ratings yet
- Cell Carcinoma, But Also To Other Cancers As Well (E.g., Thyroid Carcinoma, Melanoma)Document4 pagesCell Carcinoma, But Also To Other Cancers As Well (E.g., Thyroid Carcinoma, Melanoma)Erick EchualNo ratings yet
- 1st trimester guidelines asumDocument5 pages1st trimester guidelines asumnurfadzlin azizanNo ratings yet
- Case Study AccretaDocument35 pagesCase Study AccretaM Clarisse ParicoNo ratings yet
- Xix-A The Ethics of Ultrasound in Clinical PracticeDocument4 pagesXix-A The Ethics of Ultrasound in Clinical PracticejamiladeguzmanabcdefghijklmNo ratings yet
- Literature Review Ectopic PregnancyDocument4 pagesLiterature Review Ectopic Pregnancyakjnbowgf100% (1)
- High Risk PregnancyDocument46 pagesHigh Risk PregnancySonali SoumyashreeNo ratings yet
- Advancesinsurgeryfor Abdominalwalldefects: Gastroschisis and OmphaloceleDocument12 pagesAdvancesinsurgeryfor Abdominalwalldefects: Gastroschisis and OmphaloceleSitti HazrinaNo ratings yet
- Congenital Diaphragmatic Hernia (CDH) Information For Health ProfessionalsDocument5 pagesCongenital Diaphragmatic Hernia (CDH) Information For Health ProfessionalsMangku Liong GuanNo ratings yet
- Gynec ExamDocument45 pagesGynec ExamPutri Anggia BungaNo ratings yet
- Evan Manual ObsDocument17 pagesEvan Manual ObsAbrizan HassanNo ratings yet
- Chorionic Villi SamplingDocument8 pagesChorionic Villi SamplingDivya sharmaNo ratings yet
- Ectopic Pregnancy Literature ReviewDocument7 pagesEctopic Pregnancy Literature Reviewwgizkdvkg100% (1)
- 1060 High Risk PregnancyDocument79 pages1060 High Risk PregnancyGOPIKA C KNo ratings yet
- Amniocentesis Cbsebiology4uDocument12 pagesAmniocentesis Cbsebiology4uSharan GopinathNo ratings yet
- Diagnóstico Tardio de MARDocument8 pagesDiagnóstico Tardio de MARthedoctor1986No ratings yet
- Muhammad Redzwan Bin Abdullah: 081303583 Batch 25 Group E2Document66 pagesMuhammad Redzwan Bin Abdullah: 081303583 Batch 25 Group E2Suyajna JoshiNo ratings yet
- Dr. Maryam Al - Jaber Consultant, Family Medicine March, 2015 Dr. Omnia Darweesh Resident, Family MedicineDocument57 pagesDr. Maryam Al - Jaber Consultant, Family Medicine March, 2015 Dr. Omnia Darweesh Resident, Family MedicineFaizyabNo ratings yet
- Guide to Pediatric Urology and Surgery in Clinical PracticeFrom EverandGuide to Pediatric Urology and Surgery in Clinical PracticeNo ratings yet
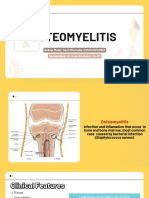
- OsteomyelitisDocument15 pagesOsteomyelitis2018B-04Desti RhomaliaNo ratings yet
- Guselkumab in Psoriatic ArthritisDocument12 pagesGuselkumab in Psoriatic ArthritisMr. LNo ratings yet
- Psychiatric History and Mental Status ExamDocument81 pagesPsychiatric History and Mental Status ExamErsido SamuelNo ratings yet
- Denial Codes 05aug2020Document9 pagesDenial Codes 05aug2020naharmampillyNo ratings yet
- Intermittent Asthma Case ReportDocument91 pagesIntermittent Asthma Case ReportCindy PrayogoNo ratings yet
- Due Date Calculator: Are You Counting Weeks, Months and Trimesters? Use Our Due Date Birthday!Document6 pagesDue Date Calculator: Are You Counting Weeks, Months and Trimesters? Use Our Due Date Birthday!Sanjay Kumar SanjuNo ratings yet
- Resultados de Búsqueda: Artículos Académicos para Vocal Function Exercises Stemple PDFDocument3 pagesResultados de Búsqueda: Artículos Académicos para Vocal Function Exercises Stemple PDFleandro__scribdNo ratings yet
- Studies On Drug Codein (MM - Ardhi Mukhoffah Bil'Ilmi 13670012)Document7 pagesStudies On Drug Codein (MM - Ardhi Mukhoffah Bil'Ilmi 13670012)ArdhieEl-ilmieNo ratings yet
- Preoperative or Pre Anaesthetic AssessmentDocument1 pagePreoperative or Pre Anaesthetic Assessmentgplabon100% (1)
- BMC Neurology 2013, 13:18Document17 pagesBMC Neurology 2013, 13:18Eliza DNNo ratings yet
- Nursing Home Lesson PlanDocument3 pagesNursing Home Lesson Planapi-353697276100% (2)
- Health Promotion "Exclusive Breast Milk"Document3 pagesHealth Promotion "Exclusive Breast Milk"Linda SaputriNo ratings yet
- The DRCOG Revision Guide Examination Preparation and Practice Questions 2nd Edition PDFDocument329 pagesThe DRCOG Revision Guide Examination Preparation and Practice Questions 2nd Edition PDFFarhan Kabir71% (7)
- Otitis MediaDocument84 pagesOtitis MediaAlex MatthewNo ratings yet
- Textbook of Medical Parasitology Provides Comprehensive CoverageDocument2 pagesTextbook of Medical Parasitology Provides Comprehensive CoverageAnge OuedraogoNo ratings yet
- Kelly Wright hw499 Unit 4 AssignmentDocument9 pagesKelly Wright hw499 Unit 4 Assignmentapi-526258935No ratings yet
- Peelings PDFDocument222 pagesPeelings PDFEdy Estévez100% (3)
- Urologic Stone Disease 2005Document51 pagesUrologic Stone Disease 2005jamilNo ratings yet
- Hiponatremia Predicts Length of Hospital Stay in ADHF PatientsDocument4 pagesHiponatremia Predicts Length of Hospital Stay in ADHF PatientsMayang Sri WulandNo ratings yet
- Drug StudyDocument6 pagesDrug StudyArdrina SappariNo ratings yet
- A Study On Effectiveness of Low Level Laser Therapy and Mcconnell Taping in Subjects With Infrapatellar BursistisDocument4 pagesA Study On Effectiveness of Low Level Laser Therapy and Mcconnell Taping in Subjects With Infrapatellar BursistisInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Republic of The Philippines Department of HealthDocument28 pagesRepublic of The Philippines Department of HealthTimothy AlmeidaNo ratings yet
- 2018 Influence of Early Physiotherapy Intervention On Pain, Joint Range of Motion and Quality of Life in Unilateral Hip Joint Replacement SurgeryDocument6 pages2018 Influence of Early Physiotherapy Intervention On Pain, Joint Range of Motion and Quality of Life in Unilateral Hip Joint Replacement SurgeryclaudiahuisachuraNo ratings yet
- Wound Care Manual, Malaysia MOHDocument199 pagesWound Care Manual, Malaysia MOHmfuadj92% (13)
- Organophosphate and Carbamate PoisoningDocument9 pagesOrganophosphate and Carbamate PoisoningFabian ClavijoNo ratings yet
- PaediatricsDocument181 pagesPaediatricsChukwuogo AkanegbuNo ratings yet
- Patient SafetyDocument27 pagesPatient Safetyarahman168No ratings yet
- Prudent Religare Employee Benefit ManualDocument24 pagesPrudent Religare Employee Benefit ManualSheikh AtifNo ratings yet
- Fendo 13 967102Document9 pagesFendo 13 967102Vilma Gladis Rios HilarioNo ratings yet
- Project in MAPEHDocument14 pagesProject in MAPEHRamel Yen CerantesNo ratings yet