You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Unit 3 DiathermyDocument63 pagesUnit 3 DiathermyAan Ika SugathotNo ratings yet
- Muscle Testing Techniques of Manual Examination PDFDocument2 pagesMuscle Testing Techniques of Manual Examination PDFIqra IftikharNo ratings yet
- Research MethodologyDocument43 pagesResearch Methodologyswaroophoppy100% (3)
- Cancer RehabDocument10 pagesCancer Rehabdrhemang100% (1)
- Active Movement and Passive MovementDocument14 pagesActive Movement and Passive MovementdrhemangNo ratings yet
- Session5 Automotive PackagingDocument72 pagesSession5 Automotive PackagingShivprasad Savadatti100% (1)
- TractionDocument6 pagesTractiondrhemang100% (1)
- Reservoir Saturation ToolDocument19 pagesReservoir Saturation ToolAli Jay JNo ratings yet
- Questions Bank On ElectrostaticsDocument2 pagesQuestions Bank On Electrostaticsashok PradhanNo ratings yet
- Qsu BriefDocument10 pagesQsu BriefdrhemangNo ratings yet
- Latest DR Hemang S Jani CVDocument5 pagesLatest DR Hemang S Jani CVdrhemangNo ratings yet
- Cardio Respiratroy Assessment FormatDocument5 pagesCardio Respiratroy Assessment FormatdrhemangNo ratings yet
- Physiotherapy Assessment for Postpartum PainDocument12 pagesPhysiotherapy Assessment for Postpartum PaindrhemangNo ratings yet
- Physiotherapy Assessment for Postpartum PainDocument12 pagesPhysiotherapy Assessment for Postpartum PaindrhemangNo ratings yet
- A Review of The Literature On Shortwave PDFDocument13 pagesA Review of The Literature On Shortwave PDFdrhemangNo ratings yet
- News & Perspective Drugs & Diseases CME & Education Log in RegisterDocument19 pagesNews & Perspective Drugs & Diseases CME & Education Log in RegisterdrhemangNo ratings yet
- Unilateral Reference Values For Hoffmann's Reflex in Patients With Suspected Lumbosacral RadiculopathiesDocument5 pagesUnilateral Reference Values For Hoffmann's Reflex in Patients With Suspected Lumbosacral RadiculopathiesdrhemangNo ratings yet
- News & Perspective Drugs & Diseases CME & Education Log in RegisterDocument19 pagesNews & Perspective Drugs & Diseases CME & Education Log in RegisterdrhemangNo ratings yet
- TocDocument2 pagesTocdrhemangNo ratings yet
- Incentive Spirometer N RESPI PNFDocument7 pagesIncentive Spirometer N RESPI PNFdrhemangNo ratings yet
- Aquatic Therapy Course at ECU Rev3Document18 pagesAquatic Therapy Course at ECU Rev3drhemangNo ratings yet
- PH.D OrdinanceDocument13 pagesPH.D Ordinancedrhemang0% (1)
- The Indian Association of PhysiotherapistsDocument6 pagesThe Indian Association of PhysiotherapistsdrhemangNo ratings yet
- Higher Algebra - Hall & KnightDocument593 pagesHigher Algebra - Hall & KnightRam Gollamudi100% (2)
- Cardiovascular Pharmacology: - Hypertension - Angina Pectoris - Cardiac Arrhythmias - Heart FailureDocument31 pagesCardiovascular Pharmacology: - Hypertension - Angina Pectoris - Cardiac Arrhythmias - Heart FailureNachiket Vijay PotdarNo ratings yet
- Introduction To Autonomic Pharmacology Part II - Anatomy ofDocument10 pagesIntroduction To Autonomic Pharmacology Part II - Anatomy ofdrhemangNo ratings yet
- Active Movement and Passive Movement (Compatibility Mode)Document3 pagesActive Movement and Passive Movement (Compatibility Mode)drhemangNo ratings yet
- Proc I Chapt 5Document18 pagesProc I Chapt 5drhemangNo ratings yet
- Bio Mechanics of The Articular CartilageDocument64 pagesBio Mechanics of The Articular CartilagedrhemangNo ratings yet
- IGCSE Chemistry TEST YOUR SELF CHAPTER 4Document12 pagesIGCSE Chemistry TEST YOUR SELF CHAPTER 4Nguyễn Việt Huy RoyNo ratings yet
- Active FilterDocument16 pagesActive FilterRam SankarNo ratings yet
- Fiber Optics Unit 3Document82 pagesFiber Optics Unit 3NIKHIL SOLOMON P URK19CS1045No ratings yet
- Heliosit OrthodonticDocument20 pagesHeliosit OrthodonticAndhika Galih PrasetyoNo ratings yet
- Búsqueda Del Medio - RENR6305 - 994F Wheel Loader Power TrainDocument5 pagesBúsqueda Del Medio - RENR6305 - 994F Wheel Loader Power TrainDavidCPNo ratings yet
- Grade 6 MathDocument12 pagesGrade 6 Mathapi-264682510No ratings yet
- E 1340 - 96 - RtezndaDocument12 pagesE 1340 - 96 - RtezndagheijoNo ratings yet
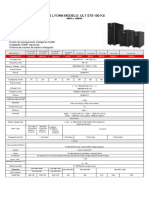
- Ups Lyonn Modelo: Ult St5-100 KS: 10KVA A 120KVADocument1 pageUps Lyonn Modelo: Ult St5-100 KS: 10KVA A 120KVASebastian Matias CruzNo ratings yet
- E16 8 2Document4 pagesE16 8 2Branko FerenčakNo ratings yet
- 20-SDMS-02 Overhead Line Accessories PDFDocument102 pages20-SDMS-02 Overhead Line Accessories PDFMehdi SalahNo ratings yet
- ELEN3017A Project Brief 2022 Rev2Document3 pagesELEN3017A Project Brief 2022 Rev2Dick MabhidaNo ratings yet
- Echotrac Mkiii: Operator'S ManualDocument48 pagesEchotrac Mkiii: Operator'S ManualKhắc PhongNo ratings yet
- FFA Furfural Fire and Health HazardsDocument2 pagesFFA Furfural Fire and Health HazardsYuga Pria PungkasanNo ratings yet
- 8 Bevel ProtractorsDocument4 pages8 Bevel Protractorssomu_amuNo ratings yet
- Financial Modelling Assignment - Ghizal Naqvi (Attock Petroleum Limited)Document13 pagesFinancial Modelling Assignment - Ghizal Naqvi (Attock Petroleum Limited)Ghizal NaqviNo ratings yet
- (Advanced Techniques For 4G Systems) : Name: Alaa Ashraf Abdelmoneim Elagrody Sec: 1 ID:1Document11 pages(Advanced Techniques For 4G Systems) : Name: Alaa Ashraf Abdelmoneim Elagrody Sec: 1 ID:1alaa elagrodiNo ratings yet
- Faculty of Engineering Mechanical Engineering Program: Vibration Engineering Lab: KM31401: LAB IVDocument7 pagesFaculty of Engineering Mechanical Engineering Program: Vibration Engineering Lab: KM31401: LAB IVhasmikaNo ratings yet
- Coreldraw 12 Hotkeys - Keyboard ShortcutsDocument6 pagesCoreldraw 12 Hotkeys - Keyboard ShortcutsRais AhmadNo ratings yet
- Review For Mastery: VocabularyDocument3 pagesReview For Mastery: VocabularyHala EidNo ratings yet
- Wiring Diagram SCH17: Service InformationDocument16 pagesWiring Diagram SCH17: Service Informationابو حمزة صبريNo ratings yet
- Electric Charges and Fields All DerivationsDocument9 pagesElectric Charges and Fields All DerivationsFlame kaiserNo ratings yet
- SMD Meter User's ManualDocument2 pagesSMD Meter User's ManuallucianoNo ratings yet
- Cambridge O Level: PHYSICS 5054/03Document16 pagesCambridge O Level: PHYSICS 5054/03Titan XosmosNo ratings yet
- Prescurtari PDFDocument67 pagesPrescurtari PDFהוד אנדרוNo ratings yet
- Problem Set Ee8205 PDFDocument4 pagesProblem Set Ee8205 PDFksajjNo ratings yet
- Compression Test/ Group 1/ Material & Science Eng'GDocument6 pagesCompression Test/ Group 1/ Material & Science Eng'GNiaz KilamNo ratings yet