You might also like
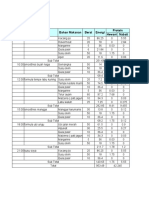
- Waktu Menu Bahan Makanan Berat Energi Protein Hewani NabatiDocument3 pagesWaktu Menu Bahan Makanan Berat Energi Protein Hewani NabatiARya SatYa AnggaraNo ratings yet
- Vitamin C Content of Guava Red MeatDocument1 pageVitamin C Content of Guava Red MeatARya SatYa AnggaraNo ratings yet
- Integrated Biological and Behavioral Surveillance Survey (IBBS) among Men who have Sex with Men (MSM) in the Kathmandu Valley - Round III Report 2009Document122 pagesIntegrated Biological and Behavioral Surveillance Survey (IBBS) among Men who have Sex with Men (MSM) in the Kathmandu Valley - Round III Report 2009ARya SatYa AnggaraNo ratings yet
- TL Report Merged Draft Ibbs 2016Document72 pagesTL Report Merged Draft Ibbs 2016ARya SatYa AnggaraNo ratings yet
- Vitamin C Content of Guava Red MeatDocument1 pageVitamin C Content of Guava Red MeatARya SatYa AnggaraNo ratings yet
- Dukungan Sosial dan Post Partum BluesDocument2 pagesDukungan Sosial dan Post Partum BluesARya SatYa AnggaraNo ratings yet
- Asian Men Who Have Sex With Men MSMs Perceptions of Risk BehaviorDocument83 pagesAsian Men Who Have Sex With Men MSMs Perceptions of Risk BehaviorARya SatYa AnggaraNo ratings yet
- Dukungan Sosial dan Post Partum BluesDocument2 pagesDukungan Sosial dan Post Partum BluesARya SatYa AnggaraNo ratings yet
- Tidur Kebutuhan KhasDocument2 pagesTidur Kebutuhan KhasARya SatYa AnggaraNo ratings yet
- CHAPTER I BroncopneumoniaDocument31 pagesCHAPTER I BroncopneumoniaARya SatYa AnggaraNo ratings yet
- Merrem IVDocument0 pagesMerrem IVhary anggoroNo ratings yet
- CHAPTER II Low Self EsteemDocument19 pagesCHAPTER II Low Self EsteemARya SatYa AnggaraNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Human Nutrition Classified Past Paper 2 Solved IGCSE Biology 0610 GCSE O LevelDocument38 pagesHuman Nutrition Classified Past Paper 2 Solved IGCSE Biology 0610 GCSE O LevelIGCSE Physics & Chemistry100% (1)
- 3.lactic Acid Fermentation of Potato Pulp by The FungusDocument4 pages3.lactic Acid Fermentation of Potato Pulp by The FungusGizemNo ratings yet
- Herbaljulie - Herbalife - Shake RecipesDocument8 pagesHerbaljulie - Herbalife - Shake Recipesapi-265490019No ratings yet
- Prospectus Syllabus: Post Graduate Diploma Course in Food Analysis and Quality AssuranceDocument19 pagesProspectus Syllabus: Post Graduate Diploma Course in Food Analysis and Quality Assurancepriyanka thapliyal100% (1)
- Ellethu Farm Feedlot Expansion PlanDocument12 pagesEllethu Farm Feedlot Expansion PlanSicelo DlaminiNo ratings yet
- Important animal feedstuffs and their classificationDocument20 pagesImportant animal feedstuffs and their classificationFAZALNo ratings yet
- Analysis: Dietary and Nutritional Approaches For Prevention and Management of Type 2 DiabetesDocument9 pagesAnalysis: Dietary and Nutritional Approaches For Prevention and Management of Type 2 DiabetesMr. LNo ratings yet
- 14 Day Fat Loss PlanDocument11 pages14 Day Fat Loss PlanAngelaNo ratings yet
- New Patient Assessment FormDocument2 pagesNew Patient Assessment Formapi-353132602No ratings yet
- Proximate Analysis Full ReportDocument26 pagesProximate Analysis Full ReportChiang Chuang Qian50% (4)
- Fine Grinding and BS3 Xylanase Improve Productivity in WeanersDocument11 pagesFine Grinding and BS3 Xylanase Improve Productivity in WeanersMilling and Grain magazineNo ratings yet
- Feed Your Flora: How To Promote Healthy Gut Bacteria: Steven Lalevich, RDDocument16 pagesFeed Your Flora: How To Promote Healthy Gut Bacteria: Steven Lalevich, RDDraganMilenkovićNo ratings yet
- Engineering Design Process for Traditional Akple FoodDocument5 pagesEngineering Design Process for Traditional Akple FoodJon KayNo ratings yet
- Research EssayDocument14 pagesResearch Essayapi-534395189No ratings yet
- Regis Benedictine Academy: Republic of The PhilippinesDocument5 pagesRegis Benedictine Academy: Republic of The PhilippinesDyanne Yssabelle DisturaNo ratings yet
- The Ultimate Meal Prep Guide in Under 40 HoursDocument18 pagesThe Ultimate Meal Prep Guide in Under 40 HoursMarcos AlvesNo ratings yet
- Tdf100a Tdfc10 en Fibra DieteticaDocument4 pagesTdf100a Tdfc10 en Fibra DieteticaRosa Karen Suarez GuzmanNo ratings yet
- Weekly Meal Plan Vol1 PDFDocument20 pagesWeekly Meal Plan Vol1 PDFSimona VacariuNo ratings yet
- Natural Pregnancy and ParentingDocument70 pagesNatural Pregnancy and ParentingAmela SabicNo ratings yet
- 14 Simple Steps To Lose 10 Pounds in A MonthDocument7 pages14 Simple Steps To Lose 10 Pounds in A MonthJaime QuinteroNo ratings yet
- JackFruit JamDocument76 pagesJackFruit JamSarkar Gattim67% (3)
- Carbohydrates Protein FatsDocument18 pagesCarbohydrates Protein Fatskristinealborte123No ratings yet
- Chapter 2 MacronutrientsDocument44 pagesChapter 2 Macronutrientsr55fsf75hp100% (1)
- Hubungan Kebiasaan Makan Makanan Rendah Serat Dengan Kejadian Apendisitis AkutDocument13 pagesHubungan Kebiasaan Makan Makanan Rendah Serat Dengan Kejadian Apendisitis Akutyuliyanti amirNo ratings yet
- Lyle McDonald - Applied Nutrition For Mixed SportsDocument77 pagesLyle McDonald - Applied Nutrition For Mixed SportsCatalin Dobre100% (11)
- MANAGING DIVERTICULITIS WITH DIET AND HYGIENEDocument5 pagesMANAGING DIVERTICULITIS WITH DIET AND HYGIENEAzyhr Htiaf Fuerzas MollionNo ratings yet
- PNABE074Document290 pagesPNABE074RyanAgungMahendraNo ratings yet
- Quantum K Healing - Newton PDFDocument157 pagesQuantum K Healing - Newton PDFJaypali Ashok Shetty100% (5)
- Eat Healthy Reading ComprehensionDocument3 pagesEat Healthy Reading ComprehensionSaid Sibouih100% (1)
- Teaching Guide 1Document80 pagesTeaching Guide 1Benito perezNo ratings yet