You might also like
- Mening-Typhoid 20apr SaudiDocument12 pagesMening-Typhoid 20apr SaudiFaizah Al GhamdiNo ratings yet
- Brucellosis - SaudiDocument16 pagesBrucellosis - SaudiFaizah Al GhamdiNo ratings yet
- Brucellosis - SaudiDocument16 pagesBrucellosis - SaudiFaizah Al GhamdiNo ratings yet
- Mening-Typhoid 20apr SaudiDocument12 pagesMening-Typhoid 20apr SaudiFaizah Al GhamdiNo ratings yet
- Anti Pyretic 2013Document15 pagesAnti Pyretic 2013Faizah Al GhamdiNo ratings yet
- SnakeDocument32 pagesSnakeFaizah Al GhamdiNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Uws Threat Hunting 101 White Paper PDFDocument25 pagesUws Threat Hunting 101 White Paper PDFJacob StamperNo ratings yet
- Luxury Hotels in PuriDocument3 pagesLuxury Hotels in PuriArjun SinghNo ratings yet
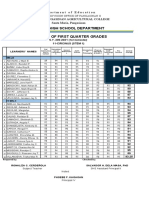
- Department of Education Senior High School 1st Quarter GradesDocument4 pagesDepartment of Education Senior High School 1st Quarter GradesRonaliza CerdenolaNo ratings yet
- Altruistic Punishment in The Classroom - Selterman (3277)Document5 pagesAltruistic Punishment in The Classroom - Selterman (3277)Laura CortesNo ratings yet
- HuDocument13 pagesHujt626No ratings yet
- Dash Kits Installation InstructionsDocument8 pagesDash Kits Installation InstructionsGeze QcoNo ratings yet
- Culture and Management in China J Child & M WarnerDocument39 pagesCulture and Management in China J Child & M WarnerCharly FezNo ratings yet
- 01.introduction To Earth ScienceDocument29 pages01.introduction To Earth ScienceIshan Chua100% (1)
- Adamson University Checklist Bachelor of Science in Architecture 2007 CurriculumDocument8 pagesAdamson University Checklist Bachelor of Science in Architecture 2007 CurriculumPinky NE OrtegaNo ratings yet
- Ie2 - Week 4 - Speaking TestDocument3 pagesIe2 - Week 4 - Speaking TestNgan TranNo ratings yet
- Stp130N6F7: N-Channel 60 V, 4.2 Mω Typ., 80 A Stripfet™ F7 Power Mosfet In A To-220 PackageDocument12 pagesStp130N6F7: N-Channel 60 V, 4.2 Mω Typ., 80 A Stripfet™ F7 Power Mosfet In A To-220 PackageOsmir MonteiroNo ratings yet
- Product Data: Carboguard 190 HDocument2 pagesProduct Data: Carboguard 190 HClarkFedele27100% (1)
- Report Part 1Document7 pagesReport Part 1Seth NurulNo ratings yet
- MC Stradale enDocument58 pagesMC Stradale enaiigee100% (2)
- Blueprints Psychiatry 6th Edition Ebook PDFDocument61 pagesBlueprints Psychiatry 6th Edition Ebook PDFpaul.tucker169100% (36)
- Focused Ion BeamDocument90 pagesFocused Ion BeamLotus DarkNo ratings yet
- Crane 3 GP160-0516-2Document222 pagesCrane 3 GP160-0516-2cengiz kutukcuNo ratings yet
- 4 Shrink Wrap - 13Document2 pages4 Shrink Wrap - 13Varun ChaitanyaNo ratings yet
- Comp 12Document36 pagesComp 12Tanu RdNo ratings yet
- t1 t2 Anglais c2013Document3 pagest1 t2 Anglais c2013Yahya AidaraNo ratings yet
- MYP Overview Integrated ScienceDocument73 pagesMYP Overview Integrated SciencerowanNo ratings yet
- MAX4208/MAX4209 Ultra-Low Offset/Drift, Precision Instrumentation Amplifiers With REF BufferDocument17 pagesMAX4208/MAX4209 Ultra-Low Offset/Drift, Precision Instrumentation Amplifiers With REF BufferAlfonso BlancoNo ratings yet
- Prestige Institute Of Management & Research IndoreDocument14 pagesPrestige Institute Of Management & Research IndoreRakesh GoliyaNo ratings yet
- Accounting IG Section 1.1 The Fundamentals of Accounting Section 1.2 The Accounting EquationDocument7 pagesAccounting IG Section 1.1 The Fundamentals of Accounting Section 1.2 The Accounting EquationJuné MaraisNo ratings yet
- Deep An GuptaDocument3 pagesDeep An GuptaArjunNo ratings yet
- Calculo Aislamiento Aisladores 10.0kVDocument8 pagesCalculo Aislamiento Aisladores 10.0kVJordi Kevin Ayala LauraNo ratings yet
- Student-Centered Learning - WikipediaDocument5 pagesStudent-Centered Learning - Wikipediajanice cipresNo ratings yet
- Judgment SheetDocument12 pagesJudgment SheetSyed AzharNo ratings yet
- 2 Basic English Vocabulary WordDocument48 pages2 Basic English Vocabulary WordMuhammad Shahbaz Shahaz SahuNo ratings yet
- Neuroscience and Biobehavioral Reviews: Cindy Stroemel-Scheder, Bernd Kundermann, Stefan Lautenbacher TDocument18 pagesNeuroscience and Biobehavioral Reviews: Cindy Stroemel-Scheder, Bernd Kundermann, Stefan Lautenbacher TAMBAR SOFIA SOTONo ratings yet