You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Assignment On Diesel Engine OverhaulingDocument19 pagesAssignment On Diesel Engine OverhaulingRuwan Susantha100% (3)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Con Men ScamsDocument14 pagesCon Men ScamsTee R TaylorNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Garrett-Satan and The Powers (Apocalyptic Vision, Christian Reflection, Baylor University, 2010)Document8 pagesGarrett-Satan and The Powers (Apocalyptic Vision, Christian Reflection, Baylor University, 2010)Luis EchegollenNo ratings yet
- TASK SHEET - Preliminary Pages of CBLMDocument2 pagesTASK SHEET - Preliminary Pages of CBLMEdleo Maghopoy80% (5)
- 20764C ENU Companion PDFDocument192 pages20764C ENU Companion PDFAllan InurretaNo ratings yet
- Flow Chart Dustin MelanconDocument1 pageFlow Chart Dustin Melanconapi-213116779No ratings yet
- Dustin FinalDocument13 pagesDustin Finalapi-213116779No ratings yet
- Budget ActivityDocument2 pagesBudget Activityapi-247490129No ratings yet
- Dustin Melancon ResumeDocument2 pagesDustin Melancon Resumeapi-213116779No ratings yet
- Peer 20 ProjectDocument1 pagePeer 20 Projectapi-213116779No ratings yet
- Sample BudgetDocument6 pagesSample Budgetapi-213116779No ratings yet
- Dustin FeedbackDocument3 pagesDustin Feedbackapi-213116779No ratings yet
- Fall EvalsDocument6 pagesFall Evalsapi-212894050No ratings yet
- December EvalDocument3 pagesDecember Evalapi-213116779No ratings yet
- Time LogsDocument2 pagesTime Logsapi-213116779No ratings yet
- Fall EvalsDocument6 pagesFall Evalsapi-212894050No ratings yet
- September Case StudyDocument16 pagesSeptember Case Studyapi-213116779No ratings yet
- Fall Semester Case LogsDocument2 pagesFall Semester Case Logsapi-213116779No ratings yet
- Fall EvalsDocument6 pagesFall Evalsapi-212894050No ratings yet
- Composite Case Study Dustin MelanconDocument32 pagesComposite Case Study Dustin Melanconapi-213116779No ratings yet
- July EvaluationDocument3 pagesJuly Evaluationapi-213116779No ratings yet
- October Case Study Dustin MelanconDocument18 pagesOctober Case Study Dustin Melanconapi-213116779No ratings yet
- CommunicationsDocument3 pagesCommunicationsapi-213427109No ratings yet
- Conference LogsDocument6 pagesConference Logsapi-213116779No ratings yet
- October EvalDocument3 pagesOctober Evalapi-213116779No ratings yet
- September EvalDocument3 pagesSeptember Evalapi-213116779No ratings yet
- July EvaluationDocument3 pagesJuly Evaluationapi-213116779No ratings yet
- June Case Study Dustin MelanconDocument19 pagesJune Case Study Dustin Melanconapi-213116779No ratings yet
- Conference LogsDocument8 pagesConference Logsapi-213116779No ratings yet
- Case Logs GraphicalDocument2 pagesCase Logs Graphicalapi-213116779No ratings yet
- July Case Study Dustin MelanconDocument19 pagesJuly Case Study Dustin Melanconapi-213116779No ratings yet
- Time LogsDocument2 pagesTime Logsapi-213116779No ratings yet
- May Case Study Dustin MelanconDocument20 pagesMay Case Study Dustin Melanconapi-213116779No ratings yet
- July EvaluationDocument3 pagesJuly Evaluationapi-213116779No ratings yet
- Semester Case StudyDocument19 pagesSemester Case Studyapi-213116779No ratings yet
- Personal Assistant With Telegram & ArduinoDocument8 pagesPersonal Assistant With Telegram & ArduinoAbhijit PattnaikNo ratings yet
- Organization and Workflow Management of Central ST PDFDocument5 pagesOrganization and Workflow Management of Central ST PDFravsab GaikwadNo ratings yet
- Mayans.M.C.S05E03.720p.WEB .x265-MiNX - SRTDocument44 pagesMayans.M.C.S05E03.720p.WEB .x265-MiNX - SRTmariabelisamarNo ratings yet
- Explain Mod 4Document20 pagesExplain Mod 4Gab IgnacioNo ratings yet
- Sanjay Chandra Vs Cbi On 23 November, 2011Document21 pagesSanjay Chandra Vs Cbi On 23 November, 2011SaiBharathNo ratings yet
- TOS-GRADE-10 EnglishDocument2 pagesTOS-GRADE-10 EnglishPRINCESS VILLASANTANo ratings yet
- Sidak 2008 FAQsDocument3 pagesSidak 2008 FAQssikhswimNo ratings yet
- Princes of the Apocalypse Locations IndexDocument2 pagesPrinces of the Apocalypse Locations IndexPedroManzelaDuarteNo ratings yet
- 1.MIL 1. Introduction To MIL Part 2 Characteristics of Information Literate Individual and Importance of MILDocument24 pages1.MIL 1. Introduction To MIL Part 2 Characteristics of Information Literate Individual and Importance of MILBernadette MendozaNo ratings yet
- 211 - Organizational Behaviour-Pearson Education Limited (2020)Document5 pages211 - Organizational Behaviour-Pearson Education Limited (2020)mozam haqNo ratings yet
- VA anesthesia handbook establishes guidelinesDocument11 pagesVA anesthesia handbook establishes guidelinesapierwolaNo ratings yet
- Breaking Bad News AssignmentDocument4 pagesBreaking Bad News AssignmentviksursNo ratings yet
- Swadhin Bangla Betar KendraDocument21 pagesSwadhin Bangla Betar KendraMusfiqur Rahman ApuNo ratings yet
- FortiEDR Product Overview TrainingDocument16 pagesFortiEDR Product Overview TrainingRafael Steven Soto del CampoNo ratings yet
- Development Through The Lifespan Test 1Document3 pagesDevelopment Through The Lifespan Test 1Alexandra CastroNo ratings yet
- French demonstrative pronouns guideDocument8 pagesFrench demonstrative pronouns guidedfñoiiuglkjs.No ratings yet
- Coursework of Signals and Systems: Moh. Kamalul Wafi December 6, 2018Document2 pagesCoursework of Signals and Systems: Moh. Kamalul Wafi December 6, 2018kartiniNo ratings yet
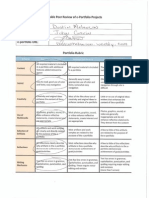
- E-Portfolio Rubric For HHS4C: Criteria Level 1 Level 2 Level 3 Level 4 Overall Expectation ADocument4 pagesE-Portfolio Rubric For HHS4C: Criteria Level 1 Level 2 Level 3 Level 4 Overall Expectation Aapi-312895913No ratings yet
- 11th Commerce Mathematics and Statistics Part II Maharashtra BoardDocument10 pages11th Commerce Mathematics and Statistics Part II Maharashtra BoardTanmay Gholap100% (3)
- SLI ProfileThe title "TITLE SLI Profile" is less than 40 characters and starts with "TITLEDocument3 pagesSLI ProfileThe title "TITLE SLI Profile" is less than 40 characters and starts with "TITLEcringeNo ratings yet
- QuitclaimDocument2 pagesQuitclaimAlfred Hernandez CampañanoNo ratings yet
- NystgmusDocument16 pagesNystgmusCheska Justine San JuanNo ratings yet
- 15 Tips To Get Fair Skin Naturally PDFDocument2 pages15 Tips To Get Fair Skin Naturally PDFLatha SivakumarNo ratings yet
- International Computer School Outlook RevisionDocument5 pagesInternational Computer School Outlook RevisionJia Hui JoanaNo ratings yet
- Automation and Artificial Intelligence in Hospitality and TourismDocument19 pagesAutomation and Artificial Intelligence in Hospitality and TourismShawn WangNo ratings yet