You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Pharmaceutical product recall guidelines summaryDocument27 pagesPharmaceutical product recall guidelines summaryAlok Kumar sharmaNo ratings yet
- Plaintiff Opposes Arbitration in Discrimination CaseDocument18 pagesPlaintiff Opposes Arbitration in Discrimination CaseAl DiamondNo ratings yet
- Patient Data Sheet: General Appearance: RespiratoryDocument5 pagesPatient Data Sheet: General Appearance: RespiratoryAshley SutherlandNo ratings yet
- CCCDocument487 pagesCCCSlaviša KovačevićNo ratings yet
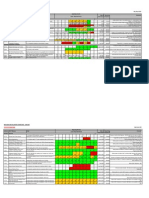
- 7.2 Balanced Scorecard App 1-9Document9 pages7.2 Balanced Scorecard App 1-9Mojtaba Andalib AzarNo ratings yet
- Health Grade 10 First QuarterDocument4 pagesHealth Grade 10 First Quarterjjggfjgh100% (3)
- Online Patient Appointment SystemDocument38 pagesOnline Patient Appointment SystemTelugu Old Movies100% (5)
- Decision Support System: by Boy S. Sabarguna, MD, Mha, PHD Jakarta, 2013Document20 pagesDecision Support System: by Boy S. Sabarguna, MD, Mha, PHD Jakarta, 2013seftiana1221No ratings yet
- Indikator Icu ElsevierDocument8 pagesIndikator Icu Elsevierseftiana1221No ratings yet
- E-Hospital - Punang Part 1Document32 pagesE-Hospital - Punang Part 1seftiana1221No ratings yet
- Clinical Decision Support System: Oleh: Dr. Dr. H. Boy S. Sabarguna, MARSDocument12 pagesClinical Decision Support System: Oleh: Dr. Dr. H. Boy S. Sabarguna, MARSseftiana1221No ratings yet
- RIsk Management UMYDocument50 pagesRIsk Management UMYseftiana1221No ratings yet
- ICu Cost EfectivenessDocument66 pagesICu Cost Efectivenessseftiana1221No ratings yet
- Dr Bambang Suryono S Healthcare ImprovementDocument54 pagesDr Bambang Suryono S Healthcare ImprovementbaskorosanjayaNo ratings yet
- E-Hospital - Punang Part 1Document32 pagesE-Hospital - Punang Part 1seftiana1221No ratings yet
- Clinical Pathway Checklist for Integrated Care PlansDocument1 pageClinical Pathway Checklist for Integrated Care Plansfidela_ffNo ratings yet
- RIsk Management UMYDocument50 pagesRIsk Management UMYseftiana1221No ratings yet
- Integrated Care PathwaysDocument64 pagesIntegrated Care Pathwaysseftiana1221No ratings yet
- Integrated Care PathwaysDocument64 pagesIntegrated Care Pathwaysseftiana1221No ratings yet
- Integrated Care PathwaysDocument64 pagesIntegrated Care Pathwaysseftiana1221No ratings yet
- Dr Bambang Suryono S Healthcare ImprovementDocument54 pagesDr Bambang Suryono S Healthcare ImprovementbaskorosanjayaNo ratings yet
- Sanatorium in GermanyDocument15 pagesSanatorium in GermanyVirginia DumitruNo ratings yet
- Groupe Mutuel Bonus SystemDocument2 pagesGroupe Mutuel Bonus SystemPrzemysław BisNo ratings yet
- DR Sagar Jawale CVDocument3 pagesDR Sagar Jawale CVSagar JawaleNo ratings yet
- From Frustration To Coping With Caring For Death by Nurse TechniciansDocument7 pagesFrom Frustration To Coping With Caring For Death by Nurse TechniciansC. R. PintoNo ratings yet
- Nursing History Timeline Key EventsDocument13 pagesNursing History Timeline Key EventsRosemarie EustaquioNo ratings yet
- Paediatric Trauma: Pauline M Cullen MBCHB FrcaDocument5 pagesPaediatric Trauma: Pauline M Cullen MBCHB FrcadamonenNo ratings yet
- NIH Public Access: Author ManuscriptDocument17 pagesNIH Public Access: Author ManuscriptJoyBoyXNo ratings yet
- Noelle Carroll Resume 3Document2 pagesNoelle Carroll Resume 3api-542966646No ratings yet
- Learnings From "Healthymagination" PDFDocument8 pagesLearnings From "Healthymagination" PDFRahulNo ratings yet
- Glaucoma and Ocular HypertensionDocument6 pagesGlaucoma and Ocular HypertensionsoniasistNo ratings yet
- Hospital Overview - Singapore General HospitalDocument2 pagesHospital Overview - Singapore General HospitalCharisma IchNo ratings yet
- Proposed 100-Bed Hospital Architectural BriefDocument2 pagesProposed 100-Bed Hospital Architectural Briefarshad khanNo ratings yet
- Model Service DeliveryDocument7 pagesModel Service DeliveryFuadNo ratings yet
- RA 9173 Phil Nursing Act of 2002Document11 pagesRA 9173 Phil Nursing Act of 2002heidivdickmanNo ratings yet
- Patan Academy of Health Sciences: Pcrlab@pahs - Edu.np Ewarsedcd@gmail - Co Pcrlab@pahs - Edu.npDocument2 pagesPatan Academy of Health Sciences: Pcrlab@pahs - Edu.np Ewarsedcd@gmail - Co Pcrlab@pahs - Edu.npBhageshwar Chaudhary100% (1)
- Ayurvedic Health & Wellness Center - Divyarishi Arogyam SansthanDocument3 pagesAyurvedic Health & Wellness Center - Divyarishi Arogyam SansthandivyarishiNo ratings yet
- 205 Principles of SafeguardingDocument16 pages205 Principles of SafeguardingUnCalatorNo ratings yet
- Professional Standards in Nursing PracticeDocument27 pagesProfessional Standards in Nursing PracticePrnce Ktn100% (2)
- Simulating Irregular Enamel Surface Texture in Composite Resin RestorationsDocument3 pagesSimulating Irregular Enamel Surface Texture in Composite Resin RestorationsIlseNo ratings yet
- An Audit of Impacted Mandibular Third Molar SurgeryDocument5 pagesAn Audit of Impacted Mandibular Third Molar SurgeryChieAstutiaribNo ratings yet
- Fluid Management BurnDocument13 pagesFluid Management BurnWeronika StarrNo ratings yet
- Central Information Commission: CIC/SA/A/2014/000004 Page 1Document32 pagesCentral Information Commission: CIC/SA/A/2014/000004 Page 1DependentNo ratings yet
- Sarala Homeopathic HospitalDocument2 pagesSarala Homeopathic HospitalSmvs Byrakur KolarNo ratings yet