You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5782)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- 6.variable V Variable F Control - Braking, Closed Loop ControlDocument25 pages6.variable V Variable F Control - Braking, Closed Loop ControlJanani RangarajanNo ratings yet
- Comparing and contrasting inductive learning and concept attainment strategiesDocument3 pagesComparing and contrasting inductive learning and concept attainment strategiesKeira DesameroNo ratings yet
- IB Diploma Maths / Math / Mathematics IB DP HL, SL Portfolio TaskDocument1 pageIB Diploma Maths / Math / Mathematics IB DP HL, SL Portfolio TaskDerek Chan100% (1)
- Presentations - Benefits of WalkingDocument1 pagePresentations - Benefits of WalkingEde Mehta WardhanaNo ratings yet
- Feminism in Lucia SartoriDocument41 pagesFeminism in Lucia SartoriRaraNo ratings yet
- Httpswww.ceec.Edu.twfilesfile Pool10j07580923432342090202 97指考英文試卷 PDFDocument8 pagesHttpswww.ceec.Edu.twfilesfile Pool10j07580923432342090202 97指考英文試卷 PDFAurora ZengNo ratings yet
- 3 QDocument2 pages3 QJerahmeel CuevasNo ratings yet
- Waiver: FEU/A-NSTP-QSF.03 Rev. No.: 00 Effectivity Date: Aug. 10, 2017Document1 pageWaiver: FEU/A-NSTP-QSF.03 Rev. No.: 00 Effectivity Date: Aug. 10, 2017terenceNo ratings yet
- Ck-Nac FsDocument2 pagesCk-Nac Fsadamalay wardiwiraNo ratings yet
- 14 Worst Breakfast FoodsDocument31 pages14 Worst Breakfast Foodscora4eva5699100% (1)
- NDA Template Non Disclosure Non Circumvent No Company NameDocument9 pagesNDA Template Non Disclosure Non Circumvent No Company NamepvorsterNo ratings yet
- Bhushan ReportDocument30 pagesBhushan Report40Neha PagariyaNo ratings yet
- Kina Finalan CHAPTER 1-5 LIVED EXPERIENCES OF STUDENT-ATHLETESDocument124 pagesKina Finalan CHAPTER 1-5 LIVED EXPERIENCES OF STUDENT-ATHLETESDazel Dizon GumaNo ratings yet
- A Chat (GPT) About The Future of Scientific PublishingDocument3 pagesA Chat (GPT) About The Future of Scientific Publishingraul kesumaNo ratings yet
- TDS Tetrapur 100 (12-05-2014) enDocument2 pagesTDS Tetrapur 100 (12-05-2014) enCosmin MușatNo ratings yet
- Climbing KnotsDocument40 pagesClimbing KnotsIvan Vitez100% (11)
- Presidential Decree 1613 Amending The Law of ArsonDocument19 pagesPresidential Decree 1613 Amending The Law of ArsonBfp Atimonan QuezonNo ratings yet
- The Role of Store LocationDocument6 pagesThe Role of Store LocationJessa La Rosa MarquezNo ratings yet
- Rock Art and Metal TradeDocument22 pagesRock Art and Metal TradeKavu RI100% (1)
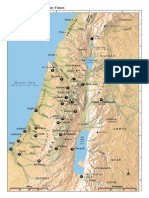
- Israel Bible MapDocument1 pageIsrael Bible MapMoses_JakkalaNo ratings yet
- MyiasisDocument29 pagesMyiasisihsanNo ratings yet
- JDDocument19 pagesJDJuan Carlo CastanedaNo ratings yet
- Basic Principles of Social Stratification - Sociology 11 - A SY 2009-10Document9 pagesBasic Principles of Social Stratification - Sociology 11 - A SY 2009-10Ryan Shimojima67% (3)
- The Hittite Name For GarlicDocument5 pagesThe Hittite Name For GarlictarnawtNo ratings yet
- Operative ObstetricsDocument6 pagesOperative ObstetricsGrasya ZackieNo ratings yet
- A Christmas Carol AdaptationDocument9 pagesA Christmas Carol AdaptationTockington Manor SchoolNo ratings yet
- E Purjee (New Technology For The Sugarcane Farmers)Document4 pagesE Purjee (New Technology For The Sugarcane Farmers)Mohammad Shaniaz IslamNo ratings yet
- Web Design Course PPTX Diana OpreaDocument17 pagesWeb Design Course PPTX Diana Opreaapi-275378856No ratings yet
- TOPIC 12 Soaps and DetergentsDocument14 pagesTOPIC 12 Soaps and DetergentsKaynine Kiko50% (2)
- Asia Competitiveness ForumDocument2 pagesAsia Competitiveness ForumRahul MittalNo ratings yet