You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- DR Ayesha - S Notes For PLAB 2Document59 pagesDR Ayesha - S Notes For PLAB 2BeaulahNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Overview of The Routine Management of The Healthy Newborn Infant - UpToDateDocument23 pagesOverview of The Routine Management of The Healthy Newborn Infant - UpToDatealwanNo ratings yet
- Case Study For Hepatitis BDocument24 pagesCase Study For Hepatitis BEmma Mariz Bernas Garcia67% (6)
- Hepatitis E VirusDocument9 pagesHepatitis E Virusapi-19880840No ratings yet
- Presentation 2Document23 pagesPresentation 2api-19880840No ratings yet
- Malaia 211Document5 pagesMalaia 211api-19880840No ratings yet
- Duration of TreamentDocument2 pagesDuration of Treamentapi-19880840No ratings yet
- Menofyia University Faculty of Nursing Nursing AdministrationDocument14 pagesMenofyia University Faculty of Nursing Nursing Administrationapi-19880840No ratings yet
- 2:induction Motor Action: Torque Induced Magnetic FieldDocument3 pages2:induction Motor Action: Torque Induced Magnetic Fieldapi-19880840No ratings yet
- Prevalence: Population at Risk For The Time Period During Which Cases CollectedDocument4 pagesPrevalence: Population at Risk For The Time Period During Which Cases Collectedapi-19880840No ratings yet
- Can Be Made at A Demographic Measures LikeDocument18 pagesCan Be Made at A Demographic Measures Likeapi-19880840No ratings yet
- AntiDocument4 pagesAntiapi-19880840No ratings yet
- World Population SituationDocument22 pagesWorld Population Situationapi-19880840No ratings yet
- Health Care System Utilization: Objectives Related To Men'S HealthDocument12 pagesHealth Care System Utilization: Objectives Related To Men'S Healthapi-19880840No ratings yet
- Effective teaching in the classهمتDocument8 pagesEffective teaching in the classهمتapi-19880840No ratings yet
- ScannerDocument64 pagesScannerapi-19880840No ratings yet
- Nursing InformaticsDocument7 pagesNursing Informaticsapi-19880840100% (1)
- Mostafa SHBLDocument1 pageMostafa SHBLapi-19880840No ratings yet
- Leg AbilityDocument28 pagesLeg Abilityapi-19880840No ratings yet
- Codes ofDocument20 pagesCodes ofapi-19880840No ratings yet
- Windows XP Professional: Qv6Vt-Xhgdk-Yq4Pv-3Gjp6-JmcpbDocument1 pageWindows XP Professional: Qv6Vt-Xhgdk-Yq4Pv-3Gjp6-Jmcpbapi-19880840No ratings yet
- AmiraDocument1 pageAmiraapi-19880840No ratings yet
- Quality Control, Quality Assurance and Total Quality Management in Construction SectorDocument220 pagesQuality Control, Quality Assurance and Total Quality Management in Construction Sectorapi-19880840No ratings yet
- CoverDocument1 pageCoverapi-19880840No ratings yet
- Immune and Molecular DiagnosticsDocument33 pagesImmune and Molecular DiagnosticsManisha PorpavaiNo ratings yet
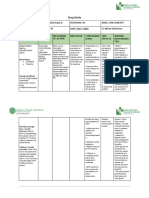
- Drug Study PDFDocument14 pagesDrug Study PDFsretirado02No ratings yet
- Hepatitis B Vaccination Status Among Students of A Medical CollegeDocument5 pagesHepatitis B Vaccination Status Among Students of A Medical CollegeDr. Imran Mahmood KhanNo ratings yet
- HIVDocument79 pagesHIVMehiella SatchiNo ratings yet
- Hepatitis B Vaccine and Immunoglobulin: Key Concepts: Review ArticleDocument7 pagesHepatitis B Vaccine and Immunoglobulin: Key Concepts: Review ArticleMarcelitaTaliaDuwiriNo ratings yet
- Hexyon LeafletDocument49 pagesHexyon LeafletEllaNo ratings yet
- Nursery Drug StudyDocument9 pagesNursery Drug StudyNiña Dianne Rubin RustiaNo ratings yet
- Dangers of The Hepatitis B VaccineDocument6 pagesDangers of The Hepatitis B Vaccinevano architectNo ratings yet
- Donor Selection 2022 DR Anoja CTPDocument80 pagesDonor Selection 2022 DR Anoja CTPchamiNo ratings yet
- IMMUNIZATION FUNDAMENTALSDocument40 pagesIMMUNIZATION FUNDAMENTALSJasmin PastoresNo ratings yet
- Needle Stick Injury and IsbarDocument29 pagesNeedle Stick Injury and Isbarkvl kandula100% (1)
- LIST OF REGISTERED DRUGS As of December 2012Document19 pagesLIST OF REGISTERED DRUGS As of December 2012Benjamin TantiansuNo ratings yet
- Vaccine Plan: The Dr. Paul ApprovedDocument9 pagesVaccine Plan: The Dr. Paul Approvedpaul popescu100% (1)
- Hepatitis B VaccineDocument6 pagesHepatitis B VaccineAziil LiizaNo ratings yet
- Engerix-B Pres Free Sds 2018-05-24Document7 pagesEngerix-B Pres Free Sds 2018-05-24anipratiwiNo ratings yet
- Hepatitis B (HepB Vaccine)Document6 pagesHepatitis B (HepB Vaccine)Desiree EscobidoNo ratings yet
- Pertussis/Whooping Cough: VACCINE - Pentavalent VaccineDocument13 pagesPertussis/Whooping Cough: VACCINE - Pentavalent VaccineLarmay dcsnNo ratings yet
- Hep B Vaccine Drug StudyDocument2 pagesHep B Vaccine Drug StudyFrian MariñasNo ratings yet
- QLD Immunisation Schedule Under 10Document2 pagesQLD Immunisation Schedule Under 10Anonymous oTObTTNo ratings yet
- Novas Diretrizes Hepatite BDocument18 pagesNovas Diretrizes Hepatite BJess jourNo ratings yet
- Turtles All The Way Down: Vaccine Science and MythDocument275 pagesTurtles All The Way Down: Vaccine Science and MythCristina CidadeNo ratings yet
- Hepa B Vaccine Consent FormDocument2 pagesHepa B Vaccine Consent FormKESLEY DELOS SANTOSNo ratings yet
- Hepatitis B and Pregnancy: An Underestimated Issue: 2009 John Wiley & Sons A/SDocument7 pagesHepatitis B and Pregnancy: An Underestimated Issue: 2009 John Wiley & Sons A/SFenny Noor AidaNo ratings yet
- EUGENICS and GENOCIDE in and From AUSTRALIA (1999) by DR Romesh Senewiratne-Alagaratnam Arya ChakravartiDocument320 pagesEUGENICS and GENOCIDE in and From AUSTRALIA (1999) by DR Romesh Senewiratne-Alagaratnam Arya ChakravartiDr Romesh Arya Chakravarti100% (1)
- Package Insert - HAVRIXDocument16 pagesPackage Insert - HAVRIXrizkaaslamNo ratings yet
- Drug Study NurseryDocument6 pagesDrug Study NurseryTanya Victoria Lean ClaudioNo ratings yet
- Pemeriksaan Terkini Hepatitis Virus: Prof. Dr. Jusak Nugraha, DR, MS, SPPK (K) Lab Patologi Klinik FK UnairDocument53 pagesPemeriksaan Terkini Hepatitis Virus: Prof. Dr. Jusak Nugraha, DR, MS, SPPK (K) Lab Patologi Klinik FK UnairMuh YunusNo ratings yet