You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Illness Biomagnetism TreatmentDocument3 pagesIllness Biomagnetism TreatmentSilvia Arias100% (2)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- CPR GuidelinesDocument30 pagesCPR GuidelineswvhvetNo ratings yet
- Orthodontics in 3 Millennia.Document7 pagesOrthodontics in 3 Millennia.ningNo ratings yet
- Dialysis in Older PatientsDocument220 pagesDialysis in Older PatientsMiguel Angel Molinero100% (1)
- Brain Gate ReportDocument31 pagesBrain Gate ReportRahul Bansal50% (4)
- Inspiration 7i Ventilator: User ManualDocument112 pagesInspiration 7i Ventilator: User ManualBiomedico UT Hospitalaria80% (5)
- Pasion ThesisDocument55 pagesPasion ThesisMagiePasion100% (1)
- Refusal To Treat A PatientDocument4 pagesRefusal To Treat A Patientzwecker4458No ratings yet
- Nerve InjuryDocument7 pagesNerve Injuryzwecker4458No ratings yet
- Detection of Cognitive Impairment in Multiple Sclerosis Based On P300 Event-Related PotentialDocument8 pagesDetection of Cognitive Impairment in Multiple Sclerosis Based On P300 Event-Related Potentialzwecker4458No ratings yet
- US Plantar FootDocument5 pagesUS Plantar Footzwecker4458No ratings yet
- Terms of The Creative Commons Attribution Share Alike-3.0 LicenseDocument78 pagesTerms of The Creative Commons Attribution Share Alike-3.0 LicenseboyzbanjarboyzNo ratings yet
- Scapular Winging PDFDocument11 pagesScapular Winging PDFzwecker4458No ratings yet
- Advance - in - Quantitative MS US Using - Texture - Analysis US Molinari2015Document14 pagesAdvance - in - Quantitative MS US Using - Texture - Analysis US Molinari2015zwecker4458No ratings yet
- Bicycle and NeuropathyDocument11 pagesBicycle and Neuropathyzwecker4458No ratings yet
- Manual Printer Driver Settings Sheet For TPP Media v05Document2 pagesManual Printer Driver Settings Sheet For TPP Media v05zwecker4458No ratings yet
- Issues in BioethicsW13Document74 pagesIssues in BioethicsW13zwecker4458No ratings yet
- Ed and Neuromodulatory MoleculesDocument6 pagesEd and Neuromodulatory Moleculeszwecker4458No ratings yet
- How to Install Custom Printer Settings in WindowsDocument3 pagesHow to Install Custom Printer Settings in Windowszwecker4458No ratings yet
- EOS Utility: Communication Software For The CameraDocument78 pagesEOS Utility: Communication Software For The CameraDepy PolNo ratings yet
- Mjud800 Stylus800 EnglishDocument166 pagesMjud800 Stylus800 EnglishKostas ChatzianastasiouNo ratings yet
- Manual Printer Driver Settings Sheet For TPP Media v05Document2 pagesManual Printer Driver Settings Sheet For TPP Media v05zwecker4458No ratings yet
- Gangguan GerakDocument31 pagesGangguan GerakFarah MuthiaNo ratings yet
- PT Assistance SyllabusDocument51 pagesPT Assistance Syllabuszwecker4458No ratings yet
- Manuel Zwecker, MD: Department of Neurological Rehabilitation, Sheba Medical Center, Tel HashomerDocument61 pagesManuel Zwecker, MD: Department of Neurological Rehabilitation, Sheba Medical Center, Tel Hashomerzwecker4458No ratings yet
- Association of Voiding Dysfunction With Functional ConstipationDocument3 pagesAssociation of Voiding Dysfunction With Functional ConstipationSisca Dwi AgustinaNo ratings yet
- Amberley Fernando: Bachelor of Science in Nutrition - Human Nutrition and Dietetics - GPA 4.0Document2 pagesAmberley Fernando: Bachelor of Science in Nutrition - Human Nutrition and Dietetics - GPA 4.0api-354220446No ratings yet
- ICH E2E GuidelineDocument20 pagesICH E2E Guidelinetito1628No ratings yet
- J7 UuurnalDocument3 pagesJ7 Uuurnalst. uswatun hasanahNo ratings yet
- Relationship Between Patients Perceptions of Care.3Document9 pagesRelationship Between Patients Perceptions of Care.3inno semuNo ratings yet
- EndokrinoDocument78 pagesEndokrinoJulian TaneNo ratings yet
- Jurnal PENDHL 1025-Article Text-1!10!20180829Document8 pagesJurnal PENDHL 1025-Article Text-1!10!20180829FZSWNo ratings yet
- Peplau's Theory of Interpersonal Relations: An Alternate Factor Structure For Patient Experience Data?Document9 pagesPeplau's Theory of Interpersonal Relations: An Alternate Factor Structure For Patient Experience Data?Rila LuaduNo ratings yet
- Evans Shianne ResumeDocument2 pagesEvans Shianne Resumeapi-490664291No ratings yet
- Twin Block 3Document2 pagesTwin Block 3GisselaMaldonadoNo ratings yet
- Improving Patient Safety in Radiotherapy by Learning From Near Misses, Incidents and ErrorsDocument5 pagesImproving Patient Safety in Radiotherapy by Learning From Near Misses, Incidents and ErrorsrosanaNo ratings yet
- AE403BIOMEDICALINSTRUMENTATIONDocument2 pagesAE403BIOMEDICALINSTRUMENTATIONalwin sozaNo ratings yet
- Chandak Myocardial PDFDocument12 pagesChandak Myocardial PDFAugustusNo ratings yet
- Nonfarmakologi Behaviour ManagementDocument23 pagesNonfarmakologi Behaviour ManagementSilviana AzhariNo ratings yet
- Terapi Cairan PD Syok KardiogenikDocument27 pagesTerapi Cairan PD Syok KardiogenikSri AsmawatiNo ratings yet
- Nursing Care PlanDocument4 pagesNursing Care PlanJoshua Pascasio100% (1)
- Endovascular Aneurysm CoilingDocument2 pagesEndovascular Aneurysm CoilingDr. Chaim B. Colen100% (1)
- UNIT 5 Factors Affecting The Healthcare System PDFDocument6 pagesUNIT 5 Factors Affecting The Healthcare System PDFDana kristenNo ratings yet
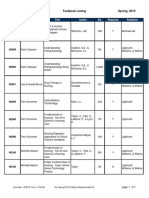
- BFLSON Course Textbook ListingDocument7 pagesBFLSON Course Textbook ListingWina ViqaNo ratings yet
- 2015 Sigmoid DiverticulitisDocument11 pages2015 Sigmoid DiverticulitisDinNo ratings yet
- Dissociative Identity DisorderDocument6 pagesDissociative Identity DisorderElean Dash Mae Abatol0% (2)
- A Case of Sarcoidosis Cured With HomoeopathyDocument3 pagesA Case of Sarcoidosis Cured With HomoeopathyDr. Rajneesh Kumar Sharma MD HomNo ratings yet
- TENSProtocolby DR Deirdre WalshDocument15 pagesTENSProtocolby DR Deirdre WalshGuy Hill100% (1)