You might also like
- Report of Anp Icu PostingDocument5 pagesReport of Anp Icu PostingsimonjosanNo ratings yet
- Cardiothoracic SurgeryDocument24 pagesCardiothoracic SurgerySimon JosanNo ratings yet
- Cardiac Surgery and InvestigationDocument30 pagesCardiac Surgery and InvestigationSimran JosanNo ratings yet
- A Comparison of Thoracic or Lumbar Patient Controlled Epidural Analgesia Methods After Thoracic SurgeryDocument12 pagesA Comparison of Thoracic or Lumbar Patient Controlled Epidural Analgesia Methods After Thoracic SurgerySimon JosanNo ratings yet
- LESSON PLAN ON Hypertension Post Basic - SC I YrDocument4 pagesLESSON PLAN ON Hypertension Post Basic - SC I Yrsimonjosan100% (1)
- Curriculum FOR B.Sc. Nursing CourseDocument133 pagesCurriculum FOR B.Sc. Nursing Coursesimonjosan100% (1)
- FEVERDocument8 pagesFEVERSimran JosanNo ratings yet
- Cardiac SurgeryDocument19 pagesCardiac SurgerySimon JosanNo ratings yet
- Beating Surgery FinalDocument17 pagesBeating Surgery FinalSimon JosanNo ratings yet
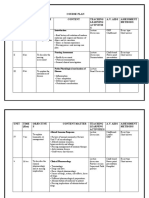
- Unit Plan UNI T Time (HRS) Objectives Content Teaching Learning Activities A.V. Aids Assessment MethodsDocument4 pagesUnit Plan UNI T Time (HRS) Objectives Content Teaching Learning Activities A.V. Aids Assessment MethodsSimran Josan100% (1)
- Nursing Process and Care PlansDocument2 pagesNursing Process and Care PlansSimran Josan63% (8)
- Lesson Plan On Myocardial InfarctionDocument14 pagesLesson Plan On Myocardial Infarctionsimonjosan90% (10)
- Course of Instruction Third Year B.Sc. Nursing Theory Sr. No. Subject Class Lab Practical Hrs. HrsDocument3 pagesCourse of Instruction Third Year B.Sc. Nursing Theory Sr. No. Subject Class Lab Practical Hrs. HrsSimran JosanNo ratings yet
- Unit Plan MSC 1 FRST Year - Docx 22Document5 pagesUnit Plan MSC 1 FRST Year - Docx 22Simran JosanNo ratings yet
- Course Plan Unit Time (HRS) Objective S Content Teaching Learning Activitie S A.V. Aids Assessment MethodsDocument8 pagesCourse Plan Unit Time (HRS) Objective S Content Teaching Learning Activitie S A.V. Aids Assessment MethodsSimran JosanNo ratings yet
- Lesson Plan On Cerebro Vascular Accident 1Document13 pagesLesson Plan On Cerebro Vascular Accident 1simonjosan67% (3)
- Lesson Plan On Myocardial InfarctionDocument14 pagesLesson Plan On Myocardial Infarctionsimonjosan90% (10)
- LESSON PLAN ON CommunicationDocument11 pagesLESSON PLAN ON CommunicationSimran Josan100% (5)
- Nursing Process and Care PlansDocument2 pagesNursing Process and Care PlansSimran Josan63% (8)
- Effective Leadership and Management Skills: Charles CotterDocument84 pagesEffective Leadership and Management Skills: Charles CottersimonjosanNo ratings yet
- LESSON PLAN ON Hypertension Post Basic - SC I YrDocument4 pagesLESSON PLAN ON Hypertension Post Basic - SC I Yrsimonjosan100% (1)
- LESSON PLAN ON CommunicationDocument11 pagesLESSON PLAN ON CommunicationSimran Josan100% (5)
- Leadership & Management of TeamsDocument30 pagesLeadership & Management of TeamssimonjosanNo ratings yet
- Lesson Plan On Cerebro Vascular Accident 1Document13 pagesLesson Plan On Cerebro Vascular Accident 1simonjosan67% (3)
- Introduction About SelfDocument27 pagesIntroduction About SelfsimonjosanNo ratings yet
- Lesson Plan: Class: Subject: Topic: Submitted byDocument10 pagesLesson Plan: Class: Subject: Topic: Submitted bysimonjosan67% (3)
- Job Application MaterialsDocument6 pagesJob Application Materialsapi-372157705No ratings yet
- Curriculum FOR B.Sc. Nursing CourseDocument133 pagesCurriculum FOR B.Sc. Nursing Coursesimonjosan100% (1)
- FEVERDocument8 pagesFEVERsimonjosanNo ratings yet
- Introduction About SelfDocument27 pagesIntroduction About SelfsimonjosanNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- PL MMF 03082022Document207 pagesPL MMF 03082022Apj MMFNo ratings yet
- Running Head: Dulaglutide 1: Dr. Angela SaathoffDocument9 pagesRunning Head: Dulaglutide 1: Dr. Angela SaathoffrhinoNo ratings yet
- List of drugs containing ephedrine and pseudoephedrineDocument1 pageList of drugs containing ephedrine and pseudoephedrineRahman PradikaNo ratings yet
- Sdcep Management of Dental Patients Taking Anticoagulants or Antiplatelet Drugs 2nd EditionDocument58 pagesSdcep Management of Dental Patients Taking Anticoagulants or Antiplatelet Drugs 2nd EditionMeryem LahlouNo ratings yet
- TABLE 132 - Recreational Substances - Intoxication WithdrawalDocument3 pagesTABLE 132 - Recreational Substances - Intoxication WithdrawalDragutin PetrićNo ratings yet
- ASEAN Variation Guideline For Pharmaceutical Products (R1) PDFDocument47 pagesASEAN Variation Guideline For Pharmaceutical Products (R1) PDFJamaila GanozaNo ratings yet
- Generic PPT 5807 5808Document23 pagesGeneric PPT 5807 5808Angel BeronioNo ratings yet
- Drugs Acting On The Cardiovascular SystemDocument12 pagesDrugs Acting On The Cardiovascular Systemcleahis cruzNo ratings yet
- CLINICAL PHARMACY ERRORSDocument30 pagesCLINICAL PHARMACY ERRORSP.S.VP JahnaviNo ratings yet
- MATERIAL LISTDocument245 pagesMATERIAL LISTRey AndreasNo ratings yet
- LVS Chronic Pain WsDocument49 pagesLVS Chronic Pain WsdtncorreoNo ratings yet
- CTD (Form 5F) : Section Sub-Section HeadingDocument19 pagesCTD (Form 5F) : Section Sub-Section Headinganon_3034696030% (1)
- Report Peer Reviewed - 2008 - Introduction To PK PD Modelling - With Focus On PK and Stochastic Differential EquationsDocument37 pagesReport Peer Reviewed - 2008 - Introduction To PK PD Modelling - With Focus On PK and Stochastic Differential EquationsOttoperritoNo ratings yet
- Lecture 1 PharmacodynamicsDocument55 pagesLecture 1 PharmacodynamicsAuthor Nauman ShadNo ratings yet
- New Drug List 1961 To Feb 2014 Pharmadocx 31.03.2014Document217 pagesNew Drug List 1961 To Feb 2014 Pharmadocx 31.03.2014Neil Dahiya100% (2)
- Đề Cương Môn Tiếng Anh Chuyên NgànhDocument11 pagesĐề Cương Môn Tiếng Anh Chuyên NgànhTrần Ngọc TùngNo ratings yet
- Medication Administration Via Enteral Tube Feeding GuideDocument31 pagesMedication Administration Via Enteral Tube Feeding GuideSara Aly YoussefNo ratings yet
- Price List HnaDocument15 pagesPrice List HnaVeChrist PharmacistoLshopNo ratings yet
- Pharmacy Technician Medication Orders GuideDocument31 pagesPharmacy Technician Medication Orders GuideAlan Hao92% (12)
- Case Presentation Station 3B Drug Study ClinidineDocument6 pagesCase Presentation Station 3B Drug Study ClinidinehahahahaaaaaaaNo ratings yet
- LamotrigineDocument109 pagesLamotriginemunzirNo ratings yet
- Biology Project: TOPIC - Study of Drugs, Their Types and Alcohol Abuse To AdolescentsDocument13 pagesBiology Project: TOPIC - Study of Drugs, Their Types and Alcohol Abuse To AdolescentsSAFDAR HafizNo ratings yet
- Indent FormDocument2 pagesIndent FormDheeraj Bhatt0% (1)
- 2015 02 Overview - New Drugs of 2014Document6 pages2015 02 Overview - New Drugs of 2014modayearNo ratings yet
- CaptoprilDocument2 pagesCaptoprilJohn Louie EscardaNo ratings yet
- Analeptic DrugDocument23 pagesAnaleptic DrugKhadim Mohiuddin100% (1)
- Anesth BarashDocument6 pagesAnesth BarashIAN GABRIELLE MERCADO CUYNONo ratings yet
- HRZE (Kid's Kit), Toradol, CiprobayDocument4 pagesHRZE (Kid's Kit), Toradol, CiprobayiloveanneNo ratings yet
- Concepts and Principles of Pharmacology To Ensure Safe and Proper Use of DrugsDocument21 pagesConcepts and Principles of Pharmacology To Ensure Safe and Proper Use of DrugsBea Bianca CruzNo ratings yet
- An Overview On Fast Disintegrating Sublingual Tablets 945-2760-1-PBDocument11 pagesAn Overview On Fast Disintegrating Sublingual Tablets 945-2760-1-PBQasim AkhtarNo ratings yet