You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- 675 Principles of Drug Addiction Treatment A Research Based Guide Third EditionDocument75 pages675 Principles of Drug Addiction Treatment A Research Based Guide Third EditionVivek VatsNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The LGBT Movements Health Issues - Higher Rates of HIV/AIDS and Other STDs Among LGBT MembersDocument127 pagesThe LGBT Movements Health Issues - Higher Rates of HIV/AIDS and Other STDs Among LGBT MembersAntonio BernardNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Teenage PregnancyDocument2 pagesTeenage PregnancyKedi BoikanyoNo ratings yet
- PRE MS N2016 Ans KeyDocument33 pagesPRE MS N2016 Ans Keyaaron tabernaNo ratings yet
- BIO CBSE 12 PROJECT On HIV/AISDocument15 pagesBIO CBSE 12 PROJECT On HIV/AISAnonymous KdUrkMIyJQ73% (56)
- Accreditation Of: Health Care SystemDocument44 pagesAccreditation Of: Health Care SystemFedelyn Mae AcaylarNo ratings yet
- Teaching Medicine and Medical Ethics Using PopularDocument180 pagesTeaching Medicine and Medical Ethics Using PopularRizky AmaliahNo ratings yet
- Lesson Plan ON Congenital SyphilisDocument19 pagesLesson Plan ON Congenital SyphilisRenuga SureshNo ratings yet
- UNICEF Presentation on Its Role & Child Protection InitiativesDocument16 pagesUNICEF Presentation on Its Role & Child Protection InitiativesKrishnaveni MurugeshNo ratings yet
- PPMP Directional Plan 2017-2022 Questions ReviewedDocument10 pagesPPMP Directional Plan 2017-2022 Questions ReviewedCecilia-Aint JaojocoNo ratings yet
- Association Between Smoking Behavior and LDLDocument1 pageAssociation Between Smoking Behavior and LDLSri Nowo MinartiNo ratings yet
- 55 259Document6 pages55 259Sri Nowo MinartiNo ratings yet
- Weight-For-Age GIRLS: 2 To 5 Years (Z-Scores)Document1 pageWeight-For-Age GIRLS: 2 To 5 Years (Z-Scores)Gibson HorasNo ratings yet
- Daftar PustakaDocument1 pageDaftar PustakaSri Nowo MinartiNo ratings yet
- VancouverDocument11 pagesVancouverAndi Firman MubarakNo ratings yet
- Nkcells Further ReadDocument1 pageNkcells Further ReadSri Nowo MinartiNo ratings yet
- Abnormal Uterine Bleeding: Frequently Asked Questions FAQ095 Gynecologic ProblemsDocument3 pagesAbnormal Uterine Bleeding: Frequently Asked Questions FAQ095 Gynecologic ProblemsErwinNo ratings yet
- Cover Skripsi Bahasa InggrisDocument1 pageCover Skripsi Bahasa InggrisSri Nowo MinartiNo ratings yet
- Nephrotic Syndrome in Adults 2009Document6 pagesNephrotic Syndrome in Adults 2009Mutiara RizkyNo ratings yet
- Alcohol 10 QuestionnaireDocument1 pageAlcohol 10 Questionnaireyash_magooNo ratings yet
- 0709Document4 pages0709Sri Nowo MinartiNo ratings yet
- Frequency of Renal Stone Disease in Patients With Urinary Tract InfectionDocument3 pagesFrequency of Renal Stone Disease in Patients With Urinary Tract InfectionSri Nowo MinartiNo ratings yet
- Management of Protozoal Diarrhoea in HIV DiseaseDocument6 pagesManagement of Protozoal Diarrhoea in HIV DiseaseSri Nowo MinartiNo ratings yet
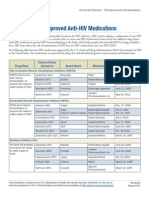
- ApprovedMedstoTreatHIV FS enDocument2 pagesApprovedMedstoTreatHIV FS enSri Nowo MinartiNo ratings yet
- Eur Heart J 2003 Fröhlich 1365 72Document8 pagesEur Heart J 2003 Fröhlich 1365 72Sri Nowo MinartiNo ratings yet
- Afroz - Lipid ProfileDocument6 pagesAfroz - Lipid ProfileSri Nowo MinartiNo ratings yet
- The Effect of Human Recombinant Erythropoietin On Prevention of Anemia of PrematurityDocument6 pagesThe Effect of Human Recombinant Erythropoietin On Prevention of Anemia of PrematuritySri Nowo MinartiNo ratings yet
- Uroanalisis AnormalDocument13 pagesUroanalisis AnormalMyke EstradaNo ratings yet
- Dysuria in AdultsDocument8 pagesDysuria in AdultsSi vis pacem...No ratings yet
- Difco BBL Mueller Hinton Agar BrothDocument5 pagesDifco BBL Mueller Hinton Agar BrothSri Nowo MinartiNo ratings yet
- Uroanalisis AnormalDocument13 pagesUroanalisis AnormalMyke EstradaNo ratings yet
- Frequency of Renal Stone Disease in Patients With Urinary Tract InfectionDocument3 pagesFrequency of Renal Stone Disease in Patients With Urinary Tract InfectionSri Nowo MinartiNo ratings yet
- ResourceDocument5 pagesResourceSri Nowo MinartiNo ratings yet
- Corrections: Theodore J. Cicero, Ph.D. Matthew S. Ellis, M.P.EDocument1 pageCorrections: Theodore J. Cicero, Ph.D. Matthew S. Ellis, M.P.ESri Nowo MinartiNo ratings yet
- Corrections: Theodore J. Cicero, Ph.D. Matthew S. Ellis, M.P.EDocument1 pageCorrections: Theodore J. Cicero, Ph.D. Matthew S. Ellis, M.P.ESri Nowo MinartiNo ratings yet
- Niacin MOADocument3 pagesNiacin MOASri Nowo Minarti100% (1)
- EpoDocument15 pagesEpoSri Nowo MinartiNo ratings yet
- Etiology and Evaluation of Diarrhea in AIDS: A Global Perspective at The MillenniumDocument10 pagesEtiology and Evaluation of Diarrhea in AIDS: A Global Perspective at The MillenniumSri Nowo MinartiNo ratings yet
- Am J Clin Nutr 2008 Kupka 1802 8Document7 pagesAm J Clin Nutr 2008 Kupka 1802 8Sri Nowo MinartiNo ratings yet
- Passmrcog Micro2016Document130 pagesPassmrcog Micro2016Cwali MohamedNo ratings yet
- Invitation LetterDocument1 pageInvitation LetterAngelo SinfuegoNo ratings yet
- Internalized Homophobia and Health Issues Affecting Lesbians and Gay MenDocument11 pagesInternalized Homophobia and Health Issues Affecting Lesbians and Gay Menushha2No ratings yet
- Requirements For An Open-Source Pharmacy Dispensing and Stores Management Software Application For Developing CountriesDocument14 pagesRequirements For An Open-Source Pharmacy Dispensing and Stores Management Software Application For Developing CountriesGFBMGFBLKNGMDSBGFNFHNFHNMHDNo ratings yet
- Fractals reveal insights into human biologyDocument5 pagesFractals reveal insights into human biologykavithanakkiran_3003No ratings yet
- Hepatitis CDocument42 pagesHepatitis Cciara sandovalNo ratings yet
- 05b HIV Testing and Counseling (National)Document26 pages05b HIV Testing and Counseling (National)AIDSPhilNo ratings yet
- Demographic Health Health SurveysDocument18 pagesDemographic Health Health SurveysERUSTUS WESANo ratings yet
- Namibia Flipchart Algorithm Child Sep2010Document11 pagesNamibia Flipchart Algorithm Child Sep2010Gabriela Morante RuizNo ratings yet
- Health: " Finally, A Medical Plan That Rewards Us For Being Healthy, and Covers Us When We Are Not! "Document7 pagesHealth: " Finally, A Medical Plan That Rewards Us For Being Healthy, and Covers Us When We Are Not! "stewartyeeNo ratings yet
- Translate UsuDocument8 pagesTranslate UsuGhina SalsabilaNo ratings yet
- Radical Philosophy 156 PDFDocument68 pagesRadical Philosophy 156 PDFkarlheinz1No ratings yet
- Ss. 11. Dr. Dhani R. Sepsis Hiv3Document43 pagesSs. 11. Dr. Dhani R. Sepsis Hiv3budi darmantaNo ratings yet
- Prevention of HerpatitisDocument54 pagesPrevention of Herpatitisapi-270822363No ratings yet
- Zubeda First Draft ThesisDocument96 pagesZubeda First Draft ThesisBereketNo ratings yet
- Chapter 21 - Aids2Document31 pagesChapter 21 - Aids2Sanjeevan Aravindan (JEEV)No ratings yet
- Gold and Nanotechnology in The Age of InnovationDocument24 pagesGold and Nanotechnology in The Age of InnovationGoldGenie AsiaNo ratings yet
- World Bank HIV/AIDS Program Development Project (II) in Nigeria, An Exploration of TB and TB/HIV OptionsDocument29 pagesWorld Bank HIV/AIDS Program Development Project (II) in Nigeria, An Exploration of TB and TB/HIV OptionsChukwu JanefrancesNo ratings yet
- 111 Laporan Kasus ToxoplasmosisDocument33 pages111 Laporan Kasus ToxoplasmosisLouis MailuhuNo ratings yet
- What Is Holding Back The Fight Against HIV/AIDS?: TimesDocument24 pagesWhat Is Holding Back The Fight Against HIV/AIDS?: TimesJohnson KwizeraNo ratings yet