You might also like
- Capnography - Self Study - GuideDocument22 pagesCapnography - Self Study - GuideSuresh KumarNo ratings yet
- Capnography: A Valuable Tool for Airway ManagementDocument17 pagesCapnography: A Valuable Tool for Airway ManagementN. TrejosNo ratings yet
- Continuous End Tidal Carbon Dioxide MonitoringDocument10 pagesContinuous End Tidal Carbon Dioxide MonitoringydtrgnNo ratings yet
- CapnographyReferenceHandbook OEM1220ADocument40 pagesCapnographyReferenceHandbook OEM1220Abayu_teNo ratings yet
- Critical Care in The Emergency Department: Monitoring The Critically Ill PatientDocument4 pagesCritical Care in The Emergency Department: Monitoring The Critically Ill PatientNurul Falah KalokoNo ratings yet
- Understanding CapnographyDocument11 pagesUnderstanding CapnographyCarolina Duque RodriguezNo ratings yet
- Monitor Carbon Dioxide with CapnographyDocument4 pagesMonitor Carbon Dioxide with CapnographysakkarashiiNo ratings yet
- CAPNOGRAPHYDocument10 pagesCAPNOGRAPHYJessica GuzmanNo ratings yet
- MU_eng_12_CapnographyDocument9 pagesMU_eng_12_Capnographykareenguallpa0No ratings yet
- Analisis de Gases SanguineosDocument18 pagesAnalisis de Gases SanguineosDiana CarolinaNo ratings yet
- Capnography 48Document18 pagesCapnography 48kota vamshiNo ratings yet
- MonitoringDocument21 pagesMonitoringalfredadevina06No ratings yet
- Capnography 1Document125 pagesCapnography 1tamikanjiNo ratings yet
- Carbon Dioxide Monitors, Exhaled GasDocument7 pagesCarbon Dioxide Monitors, Exhaled GasLee ThoongNo ratings yet
- Capnography Reference Handbook: Capnostat Loflo Flotrak Elite AccessoriesDocument40 pagesCapnography Reference Handbook: Capnostat Loflo Flotrak Elite AccessoriesLizzie RamosNo ratings yet
- ETCO2 Monitoring in Emergency SettingsDocument42 pagesETCO2 Monitoring in Emergency SettingsyennyNo ratings yet
- Capnography: July 2015Document25 pagesCapnography: July 2015Juan Manuel Medina RodriguezNo ratings yet
- M8 - Investigations and Monitoring in The ICUDocument68 pagesM8 - Investigations and Monitoring in The ICUVishal KumarNo ratings yet
- 203 1667 Applications20of20capnographyDocument25 pages203 1667 Applications20of20capnographyLusy Octavia SaputriNo ratings yet
- Time To Throw AwayDocument10 pagesTime To Throw AwayPuteri Indah Achmad HasyimNo ratings yet
- Riding The WavesDocument76 pagesRiding The WavesMedic03431No ratings yet
- Practical Use of Capnography in Exotic Animal Anesthesia: Michael Stanford, BVSC, MrcvsDocument4 pagesPractical Use of Capnography in Exotic Animal Anesthesia: Michael Stanford, BVSC, MrcvstobymusicltdNo ratings yet
- Oxygen Level Factors Affecting Barometric PressureDocument6 pagesOxygen Level Factors Affecting Barometric PressuremardatillahNo ratings yet
- 42 Respiratory Insufficiency-Pathophysiology, Diagnosis, Oxygen TherapyDocument73 pages42 Respiratory Insufficiency-Pathophysiology, Diagnosis, Oxygen TherapyLaila AcehNo ratings yet
- Clinical Measurement and EquipmentDocument29 pagesClinical Measurement and Equipmentjoe kayongoNo ratings yet
- Pulmonary function tests guideDocument24 pagesPulmonary function tests guidemerin sunilNo ratings yet
- Capnography and Its ApplicationsDocument37 pagesCapnography and Its ApplicationsTraceNo ratings yet
- Respiratory Insufficiency - Pathophysiology,: Diagnosis, Oxygen TherapyDocument11 pagesRespiratory Insufficiency - Pathophysiology,: Diagnosis, Oxygen TherapyBintang UbamnataNo ratings yet
- KapnografijaDocument9 pagesKapnografijaMarijana JakobovićNo ratings yet
- Captura de Ecrã 2024-02-07 À(s) 19.30.27Document19 pagesCaptura de Ecrã 2024-02-07 À(s) 19.30.27yurgan7No ratings yet
- Capnometry: Dhanya VDocument49 pagesCapnometry: Dhanya VdaviddanamrajanNo ratings yet
- Measurement of Gas Exchange - Pulmonary Disorders - Merck Manuals Professional EditionDocument7 pagesMeasurement of Gas Exchange - Pulmonary Disorders - Merck Manuals Professional Editionpeterpavel112No ratings yet
- The Physiology of VentilationDocument14 pagesThe Physiology of VentilationEva SánchezNo ratings yet
- Respiratory FailureDocument7 pagesRespiratory FailureJesse OnealNo ratings yet
- ETCO2 ReadingDocument19 pagesETCO2 ReadingTuan TrinhNo ratings yet
- Respiratory Failure GuideDocument29 pagesRespiratory Failure GuideberlianNo ratings yet
- Arterial Blood Gas - Treatment & Management - Point of CareDocument10 pagesArterial Blood Gas - Treatment & Management - Point of CareRo RyNo ratings yet
- Respiratory Monitoring Arterial Blood Gas Analysis Pulse Oximetry and End Tida Carbon Dioxide AnalysisDocument4 pagesRespiratory Monitoring Arterial Blood Gas Analysis Pulse Oximetry and End Tida Carbon Dioxide AnalysiskradoNo ratings yet
- ECMO Sidebotham TW Et Al ECMODocument17 pagesECMO Sidebotham TW Et Al ECMONitesh GuptaNo ratings yet
- Oxygen Saturation Monitoring With Pulse OximetryDocument9 pagesOxygen Saturation Monitoring With Pulse OximetryydtrgnNo ratings yet
- Arterial Blood Gas (ABG) AnalysisDocument5 pagesArterial Blood Gas (ABG) AnalysisDani PhilipNo ratings yet
- Insuf Respiratória Aguda - RevisãoDocument19 pagesInsuf Respiratória Aguda - RevisãoksdposaNo ratings yet
- A New Method For Noninvasive Measurement of Pulmonary Gas Exchange Using Expired GasDocument4 pagesA New Method For Noninvasive Measurement of Pulmonary Gas Exchange Using Expired GasTanmay PalNo ratings yet
- Co2测量介绍Document4 pagesCo2测量介绍Jasmine DuanNo ratings yet
- (2014) Capnography During Cardiopulmonary Resuscitation - Current Evidence and Future DirectionsDocument10 pages(2014) Capnography During Cardiopulmonary Resuscitation - Current Evidence and Future DirectionsDominik Chirito PastorNo ratings yet
- Diffusion, Blood Oxygen, Co2 EtcDocument13 pagesDiffusion, Blood Oxygen, Co2 EtcArun EbenezerNo ratings yet
- Pan 14208Document23 pagesPan 14208rizki romadaniNo ratings yet
- 2.-Oxygen Therapy and Toxicity - Paper L. MuñozDocument16 pages2.-Oxygen Therapy and Toxicity - Paper L. MuñozchascokillNo ratings yet
- Accuracy of nasal capnography in obese after surgeryDocument12 pagesAccuracy of nasal capnography in obese after surgeryFer45No ratings yet
- Camoe End-Tidal Carbon Dioxide (Etco2) : Presenter by AMO Muhamad Affendie Bin Zubir Rhu, HpupmDocument25 pagesCamoe End-Tidal Carbon Dioxide (Etco2) : Presenter by AMO Muhamad Affendie Bin Zubir Rhu, Hpupmfirdaus che daudNo ratings yet
- 10 1 1 232 716 PDFDocument17 pages10 1 1 232 716 PDFSounak BoseNo ratings yet
- Blood Gas Analysis and Acid-Base DisturbancesDocument7 pagesBlood Gas Analysis and Acid-Base Disturbancesdani2703No ratings yet
- Cap No GraphyDocument37 pagesCap No GraphyLeypotNo ratings yet
- Anesth AnalgDocument9 pagesAnesth Analgfher14bcNo ratings yet
- Tugas Inggris SukmawinataDocument2 pagesTugas Inggris SukmawinataSukma WinataNo ratings yet
- Test de Apnea - Neurocritical Care 2021Document13 pagesTest de Apnea - Neurocritical Care 2021Eva SánchezNo ratings yet
- Partial Pressure of Carbon Dioxide (PCO2) : Definition/IntroductionDocument6 pagesPartial Pressure of Carbon Dioxide (PCO2) : Definition/IntroductionRiya KumariNo ratings yet
- Bio 3 InternalsDocument16 pagesBio 3 InternalsROHAN T ANo ratings yet
- Respiratory Monitoring in Mechanical Ventilation: Techniques and ApplicationsFrom EverandRespiratory Monitoring in Mechanical Ventilation: Techniques and ApplicationsJian-Xin ZhouNo ratings yet
- David Ross - The Right and The Good (British Moral Philosophers) (2003, Oxford University Press, USA) PDFDocument242 pagesDavid Ross - The Right and The Good (British Moral Philosophers) (2003, Oxford University Press, USA) PDFwalczakc100% (1)
- Utilitarianism and BeyondDocument150 pagesUtilitarianism and BeyondDiego Mota100% (1)
- Everyday Practice of Science: Where Intuition and Passion Meet Objectivity and LogicDocument247 pagesEveryday Practice of Science: Where Intuition and Passion Meet Objectivity and LogicwalczakcNo ratings yet
- Conditional Statement and Implication PDFDocument11 pagesConditional Statement and Implication PDFwalczakcNo ratings yet
- On Being A JudgeDocument11 pagesOn Being A JudgewalczakcNo ratings yet
- Quantifying Standard of ProofDocument3 pagesQuantifying Standard of ProofwalczakcNo ratings yet
- The World of UniversalsDocument4 pagesThe World of UniversalswalczakcNo ratings yet
- Animal Rights A Critical StudyDocument45 pagesAnimal Rights A Critical StudywalczakcNo ratings yet
- ArithmeticDocument169 pagesArithmeticwalczakcNo ratings yet
- RealsDocument11 pagesRealswalczakcNo ratings yet
- Conditional Statement and Implication PDFDocument11 pagesConditional Statement and Implication PDFwalczakcNo ratings yet
- Joe and Russ discuss reason and responsibilityDocument21 pagesJoe and Russ discuss reason and responsibilitywalczakcNo ratings yet
- Paradox of ImplicationDocument12 pagesParadox of ImplicationwalczakcNo ratings yet
- Truth FunctionsDocument76 pagesTruth FunctionswalczakcNo ratings yet
- Logarithms and Their Properties Plus PracticeDocument5 pagesLogarithms and Their Properties Plus Practicedjdon12345No ratings yet
- How Stars WorkDocument65 pagesHow Stars WorkwalczakcNo ratings yet
- Contemporary MathematicsDocument295 pagesContemporary MathematicswalczakcNo ratings yet
- Geometry NotesDocument47 pagesGeometry NoteswalczakcNo ratings yet
- Intro To CV PathologyDocument13 pagesIntro To CV PathologywalczakcNo ratings yet
- Classical ConditioningDocument3 pagesClassical ConditioningFarah NoreenNo ratings yet
- Free EnergyDocument24 pagesFree EnergyVivek PattanashettiNo ratings yet
- Heavy Metal ToxDocument11 pagesHeavy Metal Toxwalczakc100% (1)
- Physics 1Document20 pagesPhysics 1walczakcNo ratings yet
- HeatDocument3 pagesHeatwalczakcNo ratings yet
- BG AnalysisDocument36 pagesBG AnalysiswalczakcNo ratings yet
- VET343 Urinary Lecture Notes 2014Document35 pagesVET343 Urinary Lecture Notes 2014walczakcNo ratings yet
- Role of Glycolysis and Respiration in Sperm Metabolism and MotilityDocument60 pagesRole of Glycolysis and Respiration in Sperm Metabolism and MotilitywalczakcNo ratings yet
- Order Out of ChaosDocument3 pagesOrder Out of ChaoswalczakcNo ratings yet
- Asimov Quick MathsDocument190 pagesAsimov Quick MathsDani Ibrahim100% (2)
- MTH114 SynotesDocument448 pagesMTH114 SynotesLloyd NarcisoNo ratings yet
- Project Report On BSNLDocument91 pagesProject Report On BSNLmanavNo ratings yet
- Sie s800 27 Sigma MiniDocument282 pagesSie s800 27 Sigma MiniHải Trần DanhNo ratings yet
- User Manual of VT310Document15 pagesUser Manual of VT310Yiditechcorp SANo ratings yet
- ChucrutDocument6 pagesChucrutPAOLANo ratings yet
- Colleen Shank Updated ResumeDocument2 pagesColleen Shank Updated Resumeapi-235595178No ratings yet
- Briefing On Attachment Programme of 72 Foundation Training CourseDocument10 pagesBriefing On Attachment Programme of 72 Foundation Training CourseSalauddinKaderNo ratings yet
- Nature's Serenity and Artistic InspirationDocument2 pagesNature's Serenity and Artistic InspirationGuilherme Daniel ColtreNo ratings yet
- Rich Text Editor For MediaWiki (Berlin, April 2010)Document16 pagesRich Text Editor For MediaWiki (Berlin, April 2010)Inez_KorczyńskiNo ratings yet
- Critique a Journal ArticleDocument2 pagesCritique a Journal ArticleRosanyanti Mokhtar100% (1)
- 2021 TAMC Roads Bridges Annual ReportDocument36 pages2021 TAMC Roads Bridges Annual ReportWXMINo ratings yet
- MODULE 1: Parts and Functions of Computers Basic Parts of ComputerDocument31 pagesMODULE 1: Parts and Functions of Computers Basic Parts of ComputerSophia Shannon D. DeiparineNo ratings yet
- Why Red Doesn't Sound Like A Bell - Understanding The Feel of Consciousness (PDFDrive)Document287 pagesWhy Red Doesn't Sound Like A Bell - Understanding The Feel of Consciousness (PDFDrive)Roger13No ratings yet
- Il Ritorno Di UliseDocument25 pagesIl Ritorno Di UliseDaniel TacheNo ratings yet
- 1-Let - Genprof - Mathematics 1-7Document8 pages1-Let - Genprof - Mathematics 1-7Rogen HemodoNo ratings yet
- Globalization and RegionalismDocument51 pagesGlobalization and RegionalismFiseha Getachew100% (1)
- B207A Powerpoint - Week 7Document25 pagesB207A Powerpoint - Week 7syed abdalNo ratings yet
- NDRRMC Update SitRep No. 7 For Typhoon KABAYAN (Muifa)Document6 pagesNDRRMC Update SitRep No. 7 For Typhoon KABAYAN (Muifa)Hiro Cerce Wilhelm ALDEN Abareta TonioNo ratings yet
- Cognitive Distortions Handout TemplateDocument3 pagesCognitive Distortions Handout TemplateLand Bank CatanauanNo ratings yet
- Vocab&GrammarDocument166 pagesVocab&GrammarWan AzliaNo ratings yet
- Bhanu Advani - Prospectus PDFDocument19 pagesBhanu Advani - Prospectus PDFBhanu AdvaniNo ratings yet
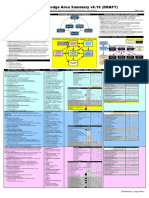
- Babok v3 Knowledge Area Summary v0.15 (DRAFT)Document2 pagesBabok v3 Knowledge Area Summary v0.15 (DRAFT)vkcon100% (1)
- DEVELOPMENT of Material ResourcesDocument21 pagesDEVELOPMENT of Material ResourcesJennifer ManaogNo ratings yet
- CPT-720 Portable Terminal Power and Environmental SpecsDocument2 pagesCPT-720 Portable Terminal Power and Environmental SpecsSantoso LeonardiNo ratings yet
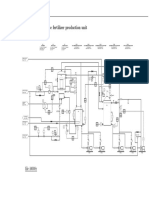
- Diagrama P ID Ammonium Nitrate Fertilizer Production Unit PDFDocument1 pageDiagrama P ID Ammonium Nitrate Fertilizer Production Unit PDFYecid Fabian AlvaradoNo ratings yet
- Unit 10: Analysis of The Business Environment of Smes: Entrepreneurship/Leadership/Innovation-MGT 2251YDocument18 pagesUnit 10: Analysis of The Business Environment of Smes: Entrepreneurship/Leadership/Innovation-MGT 2251YkiranaishaNo ratings yet
- Statistical Hydrology PDFDocument41 pagesStatistical Hydrology PDFAlexandre HesslerNo ratings yet
- Bucket Elevator Catalog PDFDocument19 pagesBucket Elevator Catalog PDFJAIRO DE JESUS JARAMILLO RAMIREZNo ratings yet
- Georg Heym The Thief and Other Stories 1Document110 pagesGeorg Heym The Thief and Other Stories 1Anna ShkodenkoNo ratings yet
- Letter From Mayor Stoney Requesting Data For Phase OneDocument2 pagesLetter From Mayor Stoney Requesting Data For Phase OneWTVR CBS 6100% (1)
- AviusDocument64 pagesAviusalex lzg100% (1)