You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Marijuana Policy Progress Report 2019 Legislative UpdateDocument28 pagesMarijuana Policy Progress Report 2019 Legislative UpdateMPP100% (3)
- Drug Information Tertiary Resources GameDocument46 pagesDrug Information Tertiary Resources Gameapi-661456802No ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Petition Urging Governors To Protect Medical Cannabis AccessDocument70 pagesPetition Urging Governors To Protect Medical Cannabis AccessMPPNo ratings yet
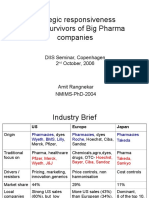
- Global Pharma StrategyDocument15 pagesGlobal Pharma StrategyDr Amit RangnekarNo ratings yet
- Severe Pain and Medical CannabisDocument1 pageSevere Pain and Medical CannabisMPPNo ratings yet
- Pediatric Practice Math ProblemsDocument3 pagesPediatric Practice Math ProblemsKaren HutchinsonNo ratings yet
- MPP Policy Paper - Regulating Cannabis Oil VaporizersDocument7 pagesMPP Policy Paper - Regulating Cannabis Oil VaporizersMPPNo ratings yet
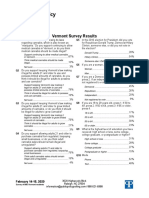
- 2020 Vermont Poll ResultsDocument7 pages2020 Vermont Poll ResultsMPPNo ratings yet
- Decriminalization and Expungement in NY: An Overview of A0840 / S06579Document1 pageDecriminalization and Expungement in NY: An Overview of A0840 / S06579MPPNo ratings yet
- Medical Cannabis Provides An Alternative To OpiatesDocument1 pageMedical Cannabis Provides An Alternative To OpiatesMPPNo ratings yet
- GQR Connecticut Poll January 2020Document1 pageGQR Connecticut Poll January 2020MPPNo ratings yet
- Medical Cannabis Implementation TimelinesDocument10 pagesMedical Cannabis Implementation TimelinesMPPNo ratings yet
- Potential Revenue From Regulating Marijuana in ConnecticutDocument2 pagesPotential Revenue From Regulating Marijuana in ConnecticutMPPNo ratings yet
- Marijuana Policy Map May 2020Document1 pageMarijuana Policy Map May 2020MPPNo ratings yet
- Simon Poll March 2019Document14 pagesSimon Poll March 2019MPPNo ratings yet
- 2018 SIU Paul Simon Public Policy Institute Legalization PollDocument4 pages2018 SIU Paul Simon Public Policy Institute Legalization PollMPPNo ratings yet
- Medical Marijuana MapDocument1 pageMedical Marijuana MapMPPNo ratings yet
- Prescribing Versus Recommending Medical CannabisDocument2 pagesPrescribing Versus Recommending Medical CannabisMPPNo ratings yet
- Maryland Progress ReportDocument2 pagesMaryland Progress ReportMPPNo ratings yet
- 2017 SIU Paul Simon Public Policy Institute Legalization PollDocument7 pages2017 SIU Paul Simon Public Policy Institute Legalization PollMPPNo ratings yet
- U.S. Attorneys' Comments Post Cole Memo RecissionDocument8 pagesU.S. Attorneys' Comments Post Cole Memo RecissionMPPNo ratings yet
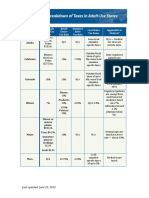
- Breakdown of Taxes in Adult-Use StatesDocument2 pagesBreakdown of Taxes in Adult-Use StatesMPPNo ratings yet
- What Does Former AG Sessions' Marijuana Enforcement Memo Mean in Practice?Document2 pagesWhat Does Former AG Sessions' Marijuana Enforcement Memo Mean in Practice?MPPNo ratings yet
- Progress Report New York Medical Marijuana ProgramDocument2 pagesProgress Report New York Medical Marijuana ProgramMPPNo ratings yet
- Sessions Asks Congress To Undo Medical Marijuana ProtectionsDocument3 pagesSessions Asks Congress To Undo Medical Marijuana ProtectionsMPPNo ratings yet
- Expungement: Removing The Life-Long Stigma Caused by Marijuana ProhibitionDocument1 pageExpungement: Removing The Life-Long Stigma Caused by Marijuana ProhibitionMPPNo ratings yet
- New Jersey Progress ReportDocument2 pagesNew Jersey Progress ReportMPPNo ratings yet
- D.C.'s Medical Marijuana ProgramDocument2 pagesD.C.'s Medical Marijuana ProgramMPPNo ratings yet
- Medical Marijuana by The NumbersDocument2 pagesMedical Marijuana by The NumbersMPPNo ratings yet
- Breakdown of Fees in Adult-Use StatesDocument6 pagesBreakdown of Fees in Adult-Use StatesMPPNo ratings yet
- Safe, Legal Access To Marijuana Can Help Fight The Opioid EpidemicDocument1 pageSafe, Legal Access To Marijuana Can Help Fight The Opioid EpidemicMPPNo ratings yet
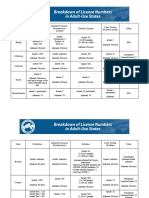
- Breakdown of License Numbers in Adult-Use StatesDocument2 pagesBreakdown of License Numbers in Adult-Use StatesMPPNo ratings yet
- Revenue From Adult Use StatesDocument5 pagesRevenue From Adult Use StatesMPPNo ratings yet
- HPLC Analysis of AcetaminophenDocument26 pagesHPLC Analysis of AcetaminophenJuan PerezNo ratings yet
- Drugs That Lower The Seizure Threshold: Andrew W HitchingsDocument10 pagesDrugs That Lower The Seizure Threshold: Andrew W HitchingsesraaNo ratings yet
- Vicp Fact SheetDocument2 pagesVicp Fact SheetDaniela OpreaNo ratings yet
- A Review On Effervescent TabletDocument6 pagesA Review On Effervescent TabletInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Chapter 10Document45 pagesChapter 10Hannah BuquironNo ratings yet
- Padma Priya Dars in I 2014Document12 pagesPadma Priya Dars in I 2014panji respatiNo ratings yet
- Rekapan Obat Dan BHP Per Distributor 14 MEIDocument25 pagesRekapan Obat Dan BHP Per Distributor 14 MEIMuhammad Yusuf UculimaNo ratings yet
- Drug PhenerganDocument1 pageDrug PhenerganSrkocherNo ratings yet
- Types of Drug Preparation (Credit To The Rightful Owner)Document1 pageTypes of Drug Preparation (Credit To The Rightful Owner)Keren Grace EspirituNo ratings yet
- General PharmacologyDocument288 pagesGeneral PharmacologyFisseha AbayNo ratings yet
- List VaksinDocument1 pageList VaksinFarmasi BSHNo ratings yet
- Principles of Drug Action 2 Barbiturate Analogs and Other Sedative Hypnotics - DeRuiter - Lecture Fall (2003) PDFDocument12 pagesPrinciples of Drug Action 2 Barbiturate Analogs and Other Sedative Hypnotics - DeRuiter - Lecture Fall (2003) PDFdextroenantiomerNo ratings yet
- Parenteral Dosage Form: Calculating Drug DosagesDocument14 pagesParenteral Dosage Form: Calculating Drug DosagesVon Valentine MhuteNo ratings yet
- IOT Rapid Sequence Induction and Intubation 2010Document8 pagesIOT Rapid Sequence Induction and Intubation 2010fe53No ratings yet
- Form Lap. Triwulan Obat PKM Dari IFKDocument11 pagesForm Lap. Triwulan Obat PKM Dari IFKWid NMNo ratings yet
- Nurdr Right To Medication QuestionsDocument6 pagesNurdr Right To Medication QuestionsSHEENA MAE DE LOS REYESNo ratings yet
- Madopar PI - 20190213 - ENDocument11 pagesMadopar PI - 20190213 - ENRonni Untung HNo ratings yet
- 3911 Human EnUserGuide Neurobion 1.3.3.2 English LeafletDocument1 page3911 Human EnUserGuide Neurobion 1.3.3.2 English LeafletNadia AfifahNo ratings yet
- Saldo Per Barang: Nama Barang Kode Barangbatch No. Exp. Datesaldo Batch Otal BarangDocument34 pagesSaldo Per Barang: Nama Barang Kode Barangbatch No. Exp. Datesaldo Batch Otal BarangimansariNo ratings yet
- Laporan Obat Fast, Slow Dan Death Moving Logistik FarmasiDocument5 pagesLaporan Obat Fast, Slow Dan Death Moving Logistik FarmasiPenunjang Medis Rs PMCNo ratings yet
- AU NZ Cortitrol PIPDocument2 pagesAU NZ Cortitrol PIPthanh.tkNo ratings yet
- Brief History of Heroin UseDocument24 pagesBrief History of Heroin UsedesmontesNo ratings yet
- Pharmacokinetics and pharmacodynamics of anaesthetic drugs in paediatricsDocument7 pagesPharmacokinetics and pharmacodynamics of anaesthetic drugs in paediatricsR KNo ratings yet
- Pyrazolone Derivatives: Rex BrogdenDocument11 pagesPyrazolone Derivatives: Rex BrogdenAnonymous 4CT2BVjVqNo ratings yet
- Total Estradiol LectureDocument68 pagesTotal Estradiol LectureLucas ElyNo ratings yet
- Adelax: Only For The Use of Medical ProfessionalsDocument2 pagesAdelax: Only For The Use of Medical Professionalsparthibanemails5779No ratings yet
- DDB Regulation No. 1 Series 2014 SummaryDocument100 pagesDDB Regulation No. 1 Series 2014 SummaryJill Marie Arabia100% (1)