You might also like
- Dental Hard Tissue Discolouration - Etiology and TreatmentDocument48 pagesDental Hard Tissue Discolouration - Etiology and TreatmentMedic PresentNo ratings yet
- Abnormalities in The Development of TeethDocument58 pagesAbnormalities in The Development of TeethAME DENTAL COLLEGE RAICHUR, KARNATAKANo ratings yet
- 2 Un-Carious Defects of TeethDocument114 pages2 Un-Carious Defects of TeethFaraz Mohammed100% (1)
- Regressive Alterations of TeethDocument25 pagesRegressive Alterations of TeethLavanya KalapalaNo ratings yet
- Root Caries by EffieDocument16 pagesRoot Caries by Effieakankiza.lucky83No ratings yet
- Cleaner Whiter Brighter! Handout 2011Document49 pagesCleaner Whiter Brighter! Handout 2011SanaFatimaNo ratings yet
- PeriodonticsDocument137 pagesPeriodonticsShawqi ANo ratings yet
- Oral Manifestations of Systemic DiseasesDocument39 pagesOral Manifestations of Systemic DiseasesAARYA100% (1)
- Discolored Teeth and Its MaagementDocument110 pagesDiscolored Teeth and Its MaagementSagarikaNo ratings yet
- Prevention of Dental Caries - 3Document49 pagesPrevention of Dental Caries - 3j6r4qvkrkzNo ratings yet
- Prevetion of Dental CariesDocument76 pagesPrevetion of Dental CariesShabeel PnNo ratings yet
- Chlorates and FluorineDocument29 pagesChlorates and FluorineElamaran AnbazhaganNo ratings yet
- Lecture VIII - PdfpedoDocument13 pagesLecture VIII - PdfpedoNoor Abdullah AlNo ratings yet
- Etiology of MalocclusionDocument46 pagesEtiology of MalocclusionMSA universityNo ratings yet
- IFDEA Dentin Hypersensitivity Educational Teaching ResourceDocument43 pagesIFDEA Dentin Hypersensitivity Educational Teaching Resourcealumera100% (1)
- Prevetion of Dental CariesDocument76 pagesPrevetion of Dental CariesmithunjithNo ratings yet
- Lecture No 1Document36 pagesLecture No 1Pawan balesara PkNo ratings yet
- Oral Systemic ConnectionDocument37 pagesOral Systemic Connectionchrisdina puspita sari100% (1)
- Presented By:: Aya Adel Abd El-Hafez Rana Mohamed EL-AbasseryDocument36 pagesPresented By:: Aya Adel Abd El-Hafez Rana Mohamed EL-AbasseryRisky Anita OktavianiNo ratings yet
- Cariology-8. Susceptible-ToothDocument36 pagesCariology-8. Susceptible-ToothVincent De AsisNo ratings yet
- Dentistry For Medical ProfessionalsDocument11 pagesDentistry For Medical ProfessionalsAnush ShahNo ratings yet
- Developmental DefectsDocument16 pagesDevelopmental DefectsdeenmNo ratings yet
- Regressive Alteration of TeethDocument29 pagesRegressive Alteration of TeethLavanya Kalapala100% (3)
- Tooth Discoloration Hypomineralization and HypoplasiaDocument5 pagesTooth Discoloration Hypomineralization and HypoplasiamirfanulhaqNo ratings yet
- Hypoplasia 1Document27 pagesHypoplasia 1Mohamed Khalil Khalil Ahmed Ellabban Ahmed EllabbanNo ratings yet
- Dentistry 101Document141 pagesDentistry 101bitiashvilinatiaNo ratings yet
- Dental stains: Causes, types and treatmentDocument30 pagesDental stains: Causes, types and treatmentArtur Radvanszki100% (1)
- Oral manifestations of Endocrine disordersDocument55 pagesOral manifestations of Endocrine disordersAkram HusseinNo ratings yet
- Oral Manifestations ShareDocument38 pagesOral Manifestations SharePrachi ChaturvediNo ratings yet
- High Yeild Conditions InbdeDocument44 pagesHigh Yeild Conditions InbdeSashwat SathishNo ratings yet
- Dental CariesDocument87 pagesDental Cariessamar yousif mohamedNo ratings yet
- Dental Caries: - DefinitionDocument82 pagesDental Caries: - DefinitionMONIKANo ratings yet
- Developmental DisordersDocument36 pagesDevelopmental DisordersANJINo ratings yet
- PEDIATRIC PATHOLOGY TITLEDocument27 pagesPEDIATRIC PATHOLOGY TITLERayne GelleNo ratings yet
- Abnormalities of TeethDocument74 pagesAbnormalities of Teethzainab.yasinNo ratings yet
- Attachment 1627848101Document33 pagesAttachment 1627848101عمار المغوارNo ratings yet
- Regressive Alteration of TeethDocument29 pagesRegressive Alteration of TeethDrRobin SabharwalNo ratings yet
- Dental Trauma Guide for Pediatric ERDocument5 pagesDental Trauma Guide for Pediatric ERt.babyNo ratings yet
- OralDocument61 pagesOralPragatiNo ratings yet
- Concepts On Metabolism, Nutrition and Endocrine FunctionDocument57 pagesConcepts On Metabolism, Nutrition and Endocrine FunctionJeanette PinkihanNo ratings yet
- Dental Caries: by DR: Hanan Eid GamalDocument107 pagesDental Caries: by DR: Hanan Eid Gamalruchika100% (1)
- Pedodontic EndodonticDocument141 pagesPedodontic EndodonticMihaela TuculinaNo ratings yet
- Dental EmergencyDocument78 pagesDental EmergencyCak Basit100% (1)
- Genetic Disorders and SyndromesDocument77 pagesGenetic Disorders and Syndromesفاطمة الجش.No ratings yet
- Anomalies DentinDocument19 pagesAnomalies DentinHaffie HafiziNo ratings yet
- Chapter 41.Ppt HypersensitivityDocument63 pagesChapter 41.Ppt HypersensitivityMaria Mercedes LeivaNo ratings yet
- Trigger Reviews: Presented by GROUP "6"Document16 pagesTrigger Reviews: Presented by GROUP "6"Bibek RajNo ratings yet
- Understanding PeriodontitisDocument67 pagesUnderstanding PeriodontitisTristan Ingrid Del ValleNo ratings yet
- Discoloration of TeethDocument5 pagesDiscoloration of Teethريام الموسويNo ratings yet
- (Bleaching) : Management of Discoloured TeethDocument40 pages(Bleaching) : Management of Discoloured TeethHari PriyaNo ratings yet
- Developmental Anomlies, Age Changes of TeethDocument61 pagesDevelopmental Anomlies, Age Changes of TeethsethupathiNo ratings yet
- Dental Caries Part 1 2020727193510Document17 pagesDental Caries Part 1 2020727193510Ayushi GoelNo ratings yet
- Oral MedicineDocument151 pagesOral Medicinedea_p27No ratings yet
- CLCPDocument43 pagesCLCPeviltohuntNo ratings yet
- Here are the steps1. Pick up your dental issue from the supply room2. Identify and organize instruments needed3. Lubricate handpieces4. Meet back here at 1pm sharp!Have fun learning! See you all laterDocument48 pagesHere are the steps1. Pick up your dental issue from the supply room2. Identify and organize instruments needed3. Lubricate handpieces4. Meet back here at 1pm sharp!Have fun learning! See you all lateryeajoon04No ratings yet
- Chapter 9 Oral Manifestations of Systemic DiseaseDocument11 pagesChapter 9 Oral Manifestations of Systemic Diseaseapi-629385674No ratings yet
- Parathyroid Gland Disorders and Their Oral ManifestationsDocument36 pagesParathyroid Gland Disorders and Their Oral ManifestationsJamesNo ratings yet
- Epidemiology of MalocclusionDocument7 pagesEpidemiology of MalocclusionAsad Khan5556No ratings yet
- Developmental Disorders of TeethDocument176 pagesDevelopmental Disorders of TeethPawan Kumar100% (5)
- Drugs in EndoDocument127 pagesDrugs in EndoMarius sNo ratings yet
- What Is Periapical PeriodontitisDocument2 pagesWhat Is Periapical PeriodontitisdeenmNo ratings yet
- 2016 Anesthesia Use GuidelinesDocument12 pages2016 Anesthesia Use GuidelinesdeenmNo ratings yet
- Medical EmergenciesDocument4 pagesMedical EmergenciesdeenmNo ratings yet
- RPD Review QuestionsDocument85 pagesRPD Review Questionsdeenm67% (3)
- Gingival InflammationDocument12 pagesGingival InflammationdeenmNo ratings yet
- Applied Biomaterials Exam 4 2007Document5 pagesApplied Biomaterials Exam 4 2007deenmNo ratings yet
- Role of Pharmacological Agents in Endodontal TherapyDocument3 pagesRole of Pharmacological Agents in Endodontal TherapydeenmNo ratings yet
- Periohistology QuizDocument6 pagesPeriohistology QuizdeenmNo ratings yet
- 5 Perio Pathogenesis08 PDFDocument9 pages5 Perio Pathogenesis08 PDFdeenmNo ratings yet
- 1024 SwellingsDocument10 pages1024 Swellingsdukedream143No ratings yet
- Oral Diagnosis and Treatment Planning: Part 7. Treatment Planning For Missing TeethDocument11 pagesOral Diagnosis and Treatment Planning: Part 7. Treatment Planning For Missing TeethalfredoibcNo ratings yet
- 1024 SwellingsDocument10 pages1024 Swellingsdukedream143No ratings yet
- Oral Squamous Cell CarcinomaDocument10 pagesOral Squamous Cell CarcinomadeenmNo ratings yet
- Plaque FluidDocument7 pagesPlaque FluiddeenmNo ratings yet
- Principles of AdhesionDocument44 pagesPrinciples of AdhesionOmar Hesham SalahNo ratings yet
- Skateboarding Injury or AbuseDocument6 pagesSkateboarding Injury or AbusemirfanulhaqNo ratings yet
- Fluoride in DentistryDocument42 pagesFluoride in DentistryAbhishek SoniNo ratings yet
- NeoplasiaDocument4 pagesNeoplasiadeenmNo ratings yet
- 53.unexpected Findings PDFDocument6 pages53.unexpected Findings PDFdeenmNo ratings yet
- 50.missing Upper Lateral IncisorsDocument4 pages50.missing Upper Lateral IncisorsmirfanulhaqNo ratings yet
- 28.A Very Painful Mouth PDFDocument4 pages28.A Very Painful Mouth PDFdeenmNo ratings yet
- 56.rapid Breakdown of First Permanent Molars PDFDocument4 pages56.rapid Breakdown of First Permanent Molars PDFmirfanulhaqNo ratings yet
- 42.will You See My SonDocument4 pages42.will You See My SonmirfanulhaqNo ratings yet
- Radiographic InterpretationDocument52 pagesRadiographic InterpretationdeenmNo ratings yet
- Self Study Intraoral Anatomy RadiologyDocument80 pagesSelf Study Intraoral Anatomy RadiologydeenmNo ratings yet
- 21.trauma To An Immature IncisorDocument4 pages21.trauma To An Immature IncisordeenmNo ratings yet
- Bilateral Facial Swelling DiagnosisDocument4 pagesBilateral Facial Swelling DiagnosisdeenmNo ratings yet
- Clinical Tooth BleachingDocument8 pagesClinical Tooth BleachingdeenmNo ratings yet
- Summary of Tooth DevelopmentDocument1 pageSummary of Tooth DevelopmentdeenmNo ratings yet
- Outline Form:: The Following Factors Govern ThemDocument10 pagesOutline Form:: The Following Factors Govern ThemZerrina EvangelistaNo ratings yet
- Permanent Mandibular CaninesDocument25 pagesPermanent Mandibular CaninesLavanya KalapalaNo ratings yet
- The Relationship Between Incisor Crown Shape and Dental CrowdingDocument6 pagesThe Relationship Between Incisor Crown Shape and Dental CrowdingAndrésAcostaNo ratings yet
- Non Surgical Endodontic Retreatment: Presented byDocument58 pagesNon Surgical Endodontic Retreatment: Presented bySayak GuptaNo ratings yet
- 10 Review JaiswalDocument7 pages10 Review JaiswalAniket PotnisNo ratings yet
- 1 Classification of Extensively Damaged Teeth To Evaluate Prognosis - JCDA - Essential Dental KnowledgeDocument9 pages1 Classification of Extensively Damaged Teeth To Evaluate Prognosis - JCDA - Essential Dental KnowledgeA Aran PrastyoNo ratings yet
- Scopin 2019 Carillas PerioDocument15 pagesScopin 2019 Carillas PeriojotapintorNo ratings yet
- Introduction To PedodonticsDocument29 pagesIntroduction To PedodonticsBanyu علي تقويم Biru100% (1)
- Gummetal wire simplifies orthodontic treatmentDocument8 pagesGummetal wire simplifies orthodontic treatmentcmmbNo ratings yet
- Oral Habits and Its Relationship To Malocclusion A Review.20141212083000Document4 pagesOral Habits and Its Relationship To Malocclusion A Review.20141212083000Stacia AnastashaNo ratings yet
- Periodontal Health During Clear Aligners Treatment: A Systematic ReviewDocument5 pagesPeriodontal Health During Clear Aligners Treatment: A Systematic ReviewfaouziNo ratings yet
- PULP TESTS-converted EndodonticsDocument12 pagesPULP TESTS-converted EndodonticsWajeeha Khan KhattakNo ratings yet
- Radii Plus +: Your Choice of Accessories yDocument2 pagesRadii Plus +: Your Choice of Accessories yDimas NavarroNo ratings yet
- 18 Interrelationship of Orthodontics With Periodontics and Restorative DentistryDocument25 pages18 Interrelationship of Orthodontics With Periodontics and Restorative DentistrySriAduri100% (1)
- Determination of Vertical Characteristics With Different Cephalometric MeasurementsDocument7 pagesDetermination of Vertical Characteristics With Different Cephalometric MeasurementsAriadna MéndezNo ratings yet
- ContentServer - Asp 36Document5 pagesContentServer - Asp 36mutiaNo ratings yet
- Pattern of Partial Tooth Loss in Guntung Ujung VillageDocument6 pagesPattern of Partial Tooth Loss in Guntung Ujung VillagerahmaNo ratings yet
- Surgical Extrusion: A Dental TechniqueDocument6 pagesSurgical Extrusion: A Dental TechniqueDragos CiongaruNo ratings yet
- Desensitasi 2Document7 pagesDesensitasi 2fennilubisNo ratings yet
- Tooth Development Lecture 4Document9 pagesTooth Development Lecture 4eveNo ratings yet
- Ectopic EruptionDocument4 pagesEctopic EruptionBhumika SharmaNo ratings yet
- Avulsion and Replantation of Primary Teeth A Feasible OptionDocument3 pagesAvulsion and Replantation of Primary Teeth A Feasible OptionSushmita AlmiraNo ratings yet
- 770 QuestionsDocument88 pages770 Questionssmile4Dr76% (25)
- Furcation involvement diagnosis and classificationDocument26 pagesFurcation involvement diagnosis and classificationYehya Al KhashabNo ratings yet
- Heterodonty and Tooth Replacement Patterns in Nile CrocodilesDocument7 pagesHeterodonty and Tooth Replacement Patterns in Nile CrocodilesJorge W. Moreno BernalNo ratings yet
- Fill and Drill Technique Case Report PDFDocument10 pagesFill and Drill Technique Case Report PDFAmee PatelNo ratings yet
- Basic Periodontal ExamDocument3 pagesBasic Periodontal ExamAnonymous k8rDEsJsU1No ratings yet
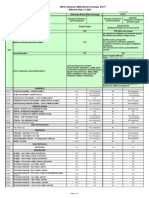
- MCS Classicare (MA) Dental Coverage SummaryDocument4 pagesMCS Classicare (MA) Dental Coverage SummaryJessicaNo ratings yet
- Clinical Features of PeriodontitisDocument36 pagesClinical Features of Periodontitislenami_91No ratings yet
- VESTIBULOPLASTY4JDocument3 pagesVESTIBULOPLASTY4JrashmitanayakNo ratings yet