DOI: 10.5958/2319-5886.2015.00129.
International Journal of Medical Research
&
Health Sciences
www.ijmrhs.com
Volume 4 Issue 3 Coden: IJMRHS
Copyright @2015
th
th
Received: 17 Feb 2015
Revised: 25 Mar 2015
Discussion
ISSN: 2319-5886
Accepted: 23rd Apr 2015
OPTIMAL eCRF DESIGN, USER FRIENDLY INTERFACE AND PROPER TRAINING:
QUINTESSENTIAL FOR HIGH QUALITY DATA IN REAL WORLD EVIDENCE (RWE) STUDIES
*RiturajMohanty1, ArunGowda2, AnupNair3, AnilSharma4, UttamBarick5
1
M.B.B.S, Associate Project Manager, 2M.B.B.S, Director, 3M.Sc, Clinical Research Associate,
4,5
M.Sc, Clinical Research Consultant, Focus scientific research center (FSRC), part of phamax AG, #19 KMJ
Ascend, 17th C Main, 1st Cross, 5th Block, Koramangala, Bengaluru, Karnataka, India 560095.
* Corresponding author email: rituraj.mohanty@fs-researchcenter.com
ABSTRACT
Background: The success of a Real World Evidence (RWE) study lies in collecting and processing high quality
data. Data in RWE study can be collected in a paper format as in a Case Report Form (CRF) or electronically in
the format of electronic Case Report Form (eCRF). For a multi-country/multi-centric study, eCRF can offer
advantages over the conventional paper CRF for collection of data. An approach which is a combination of
optimal eCRF design, user friendly interface and proper training can facilitate in collection of high quality data.
Aim: The aim of this article is to highlight the significance of optimal eCRF design, user friendly interface and
proper training in RWE studies. Conclusion: Implementation of EDC system with eCRF can be advantageous for
a multi-country/multi-centric RWE studies, as it facilities real time monitoring, which can yield adequate data of
high quality. Implementation of eCRF can be cost and time effective.
Keywords: Electronic Case Report Form (eCRF), Electronic Data Capture (EDC), Patient Registry, Real World
Evidence (RWE), Stakeholders
INTRODUCTION
A patient registry (an example of RWE study) is an
organized system that uses observational study
methods to collect uniform data to evaluate specified
outcomes for a population defined by a particular
disease, condition, or exposure, and that serves one or
more predetermined scientific, clinical, or policy
purposes. If designed and conducted properly it can
provide useful data on the real-world view of clinical
practice, patient outcomes, safety and comparative
effectiveness [1]. Apart from the study protocol the
most important element of a RWE study is the tool
designed and used to collect data. CRFs and
questionnaires have been traditionally used for
collecting data in clinical studies. Data collection in
CRF though simple is time-consuming, tedious and
error prone [2]. Moreover in cases where the study is
spread over a larger geographical area, the logistics
associated with paper based CRF is substantial and
cumbersome. An Electronic Data Capture (EDC)
system is a computerized system designed for the
collection of clinical data in electronic format.
EDC system typically has eCRF, which is basically
the CRF in electronic format into which data is
populated directly with the help of an appropriate
browser. The convenience of eCRF from data
collection point of view is that the data can be
monitored and evaluated in real time. The system
allows the study monitor to access anonymous data
from centers throughout the study duration and check
them on a real time basis. A well designed eCRF also
has numerous edit checks within itself, thereby
675
Rituraj et al.,
Int J Med Res Health Sci. 2015;4(3):675-679
prompting the investigator/end user if the data
entered is incorrect or illogical.
Some of the core features of the EDC system are
ideally characterized by:
1. Different levels of user access so that data can be
monitored at multiple levels
2. Secured platform with password protection and
validated by electronic signatures
3. Facilitates remote data capture and real time
monitoring
4. Reduced data redundancy as data captured once
is populated in relevant fields
5. Facilitates real time query management thus
reducing total turnout time
6. Generation of reports which has data on
recruitment and other parameters
7. Central storage of anonymous data with back up
8. Automation leading to faster study start up and
closure
9. Early database lock leading to timely study
completion [3]
10. Cost effective as compared to paper based CRF
in certain scenarios [4]
eCRF Design; Designing the eCRF is a critical step
in conduct of a RWE study. Contrary to randomized
clinical trials, generally, in RWE studies or patient
registries, the protocol does not mandate the
investigator for any intervention. The investigator
collects and populates patient data as per the standard
clinical practice and local guidelines/regulations. A
particular RWE study conducted on a multi-country,
multi-centric platform involving data collection from
different geographical regions typically follows a
trend specific to local practices and requirements of
that particular region. Keeping the above in view,
optimal eCRF design becomes quintessential if the
right amount and right quality of data have to be
collected to yield meaningful analysis and results.
The fundamental basis of eCRF design is that it
should ideally be FDA 21 CFR Part 11 compliant
[5,6]
.It should also have appropriate internal and
external security safeguards [7].The operations team
ideally plays a crucial role in the design and
validation of the eCRF. The team responsible for
designing the database and eCRF should receive the
study protocol as soon as possible and the initiation
of eCRF design need not wait for the protocol to be
finalized, but can start in parallel to the review and
finalization of the protocol. The data parameters
derived ideally from the protocol are listed down,
logically segregated into sections/visits and
transcribed into paper CRF. The CRF should undergo
thorough review by clinical/scientific experts to make
sure that all the data parameters necessary to satisfy
the data requirements of the primary and secondary
objectives/outcomes of the protocol are considered
and included. An easy to use eCRF, both from an
investigator and a data analyst perspective is one that
has maximal drop down menus and radio
buttons/check boxes for collection of data and
minimal free text entry. End-to-end testing of the
eCRF portal is critical. The eCRF should be
rigorously tested by populating dummy data and all
types of user scenarios to ensure that all real life
events are considered and replicated without any
errors. The training eCRF portal should be fully
tested, validated and approved before release.
Training needs to be delivered to individual
investigators and all other end users identified at that
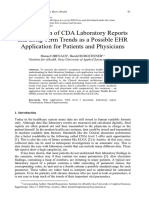
stage of the study. Indicative approach to eCRF
designing is outlined in Figure 1. To maintain the
sanctity of data and restrict the access to various
types of functionality on the eCRF portal, relevant
user specific access rights should be generated and
provided as agreed and approved between the sponsor
and other stakeholders. Despite best trainings, a user
guide should be made available to the respective sites
and other stakeholders.
User Interface: No matter how technically correct
the eCRF portal might be, it fails to serve its purpose
if the investigators/end users find it difficult to use.
The interface needs to have the following basic
components which would make it widely acceptable
in studies which are conducted across the world
within multi-cultural setups:
1. Compatibility with different browsers
2. Minimal hardware requirements
3. Minimal internet bandwidth requirement
4. Simple log in and log out procedures
5. Dedicated drop down menus or icons for different
functionalities
6. Ease of toggling from page to page
7. Secure and easily retrievable password protection
8. Help option next to login screen listing frequently
encountered eCRF issues with possible resolutions
9. Clear and simple user guide with local language
support
10. 24 hour helpdesk to solve any technical queries
676
Rituraj et al.,
Int J Med Res Health Sci. 2015;4(3):675-679
Acceptability of the eCRF portal is enhanced if the
investigators/end users find it simple and uncluttered.
One of the important aspects of the interface is that it
should have provision for remote access by the
technical team in case the investigator/end user
encounters difficulties in populating data or using any
of the functionalities.
Fig 1: Schematic approach to eCRF design and validation (indicative only)
Training: A very important aspect of the entire
activity is ensuring that the investigators/end users
are properly trained and understand how to use the
eCRF portal.
It is quite common to encounter some level of
resistance and hesitancy from a handful of
investigators towards the eCRF approach of data
collection. It is always better to identify such
investigators prior to their enrolment on the study.
Some investigators express their resistance towards
eCRF once the study has been initiated and patient
enrolments are on-going. Hence, the eCRF training
sessions should also encompass a module which
clearly enumerates the reasons why this study is on
eCRF and the benefits it provides to all in terms of
time, efforts, money and the ease of conducting
studies. Wherever required and applicable, a case
study objectively portraying these variables in
tangible terms and/or numeric values should always
be targeted. Such portrayal has a tendency to simplify
the explanations and hence can have a higher
probability of connecting with the intended audience
who are mostly physicians.
Trainings, however good should never be a
standalone activity. Trainings for a longer duration
study or for those studies where numerous changes
are consistently incorporated in the protocol/eCRF
needs to be repetitive in nature. Such repeat sessions
may not necessarily be face to face but can be web
based interactive sessions with voice support and live
video transmission wherever applicable/possible.
Repeat training for minor updates in protocol
affecting the eCRF data collections can also be
scheduled using the simple teleconference mode.
The trainer needs to be well prepared and equipped
with all the support documents and tools necessary to
impart such training sessions effectively. The list of
frequently asked questions (FAQs) should always be
shared well in advance with the sites/
investigators/end users along with the technical
requirements documents. The trainer should always
know the targeted audiences linguistic and cultural
gaps. Based on this assessment if the services of
interpreters are necessary then they should be
appointed for the training sessions and the relevant
audience informed of the same well before the start of
the session.
The training session needs to have inbuilt checks and
balances to periodically assess whether the training
serves its intended purpose and the audience is able to
well comprehend the contents. This can be done
through frequent questions on whatever has been
discussed till that point and getting an
online/telephonic feedback based responses. Based on
the responses gathered, the trainer should always
assess any gaps in the understanding of the audience
and modulate his/her further sessions/slides
accordingly. During remote trainings it is always
sought that the training platforms login credentials
have been first shared with all. It should be ensured
677
Rituraj et al.,
Int J Med Res Health Sci. 2015;4(3):675-679
that all have successfully logged into it and proceed
on that platform with the new dummy data entries as
per the training document pre-shared with them. The
trainer should always ensure that the pace maintained
for the trainings never exceed beyond a point even if
audience seems very receptive. Neither should it be
too slow to keep pace with slow learners as this can
trigger negative interests among the bulk of those
who have been receptive and in sync with the trainer.
If required, the trainer can conduct an additional
session with the slow learners on need basis. The
option of submitting questions should always be
incorporated. All the questions collated by the end of
the session should be answered. If the time doesnt
permit to discuss all the questions, then the trainer
should request them to submit their remaining
questions and assure them of a time bound email
based response. The trainer should maintain a
question and answer log of that session and share it
within a specified time period post training with all
the audience via email. The trainer should also share
his/her contact details with them for any future
correspondence or queries related to the training
imparted and must ensure that prompt responses are
provided to all correspondences.
DISCUSSION
With ever increasing need of more data and better
data by pharmaceutical companies and other
stakeholders involved, the future of EDC system
seems promising. Technology has bridged the gap
between different stakeholders promoting their active
participation in any particular study. Newer devices
and interfaces are being developed at a rapid rate and
the EDC system will have to keep pace with them in
order to be compatible. As the acceptability of
technology increases, EDC systems will have to be
made device and platform agnostic. The EDC system
will need to evolve to provide interoperability
between differential clinical and e-health systems
among several standard consortiums [8,9]. In this
modern age of automation, large scale integration of
processes on a real time basis is desirable to obtain
credible results within justified and acceptable
timelines. Paper based CRF have been used
extensively in the past but as studies get expansive
and diversified, integration of EDC system for data
collection will be critical for study success. A study
evaluating EDC in developing country has
demonstrated that if EDC system is well designed and
introduced with care, and work processes are adjusted
to EDC, it will become a more time effective,
potentially more accurate and therefore cost effective
method than the standard paper-based data collection
method [10].
CONCLUSION
In
multi-country/multi-centric
RWE
studies,
implementation of EDC system with eCRF can be
advantageous as it facilities real time monitoring,
which can yield adequate data of high quality.
Collection of data in eCRF can be cost and time
effective. In order to encourage acceptance of
investigators/end
users
to
EDC
system,
implementation of an approach which combines
optimal eCRF design, user friendly interface and
proper training could be critical for success.
ACKNOWLEDGEMENT
The authors would like to acknowledge the efforts of
Mahafroz Khatib, Scientific Associate and Barani
Kumar, Graphic Designer at FSRC for their
invaluable support in the development of this article.
Conflict of interest: Nil
REFERENCES
1. Gliklich R, Dreyer N, Leavy M, eds. Registries
for Evaluating Patient Outcomes: A Users
Guide. Third edition. Agency for Healthcare
Research and Quality. 2014;13(14)
2. Shah J, Rajgor D, Pradhan S, McCready M,
Zaveri A, Pietrobon R. Electronic Data Capture
for Registries and Clinical Trials in Orthopaedic
Surgery: Open Source versus Commercial
Systems. ClinOrthopRelat Res.2010;468:2664
71
3. Mitchel JT, Kim YJ, Choi J, Tantsyura V, Nadler
D, Grimes I et al. The Impact of Electronic Data
Capture on Clinical Data Management:
Perspectives from the Present into the Future.
Monitor 2008. Available at: http://www. Target
health.com/PDF/Articles/11228-08_Mitchel.pdf
4. Pavlovi I, Kern T, Miklavi D. Comparison of
Paper-based and Electronic Data Collection
Process in Clinical Trials: Costs Simulation
678
Rituraj et al.,
Int J Med Res Health Sci. 2015;4(3):675-679
5.
6.
7.
8.
9.
10.
Study: Contemporary Clinical Trials.2009; 30:
300316
Ene-Iordache B, Carminati B, Antiga L, Rubis N,
Ruggenenti P, Remuzzi G, et al. Developing
Regulatory-compliant Electronic Case Report
Forms for Clinical Trials: Experience with The
Demand Trial. Journal of the American Medical
Informatics
Association.
JAMIA
2009;16(3):40408
FDA. 21 CFR Part 11: Electronic Records;
Electronic Signatures-Scope and Application.
August 2003. Available at: http://www.
fda.gov/downloads/RegulatoryInformation/Guida
nces/ucm125125.pdf
FDA. Guidance for Industry: Computerized
Systems Used in Clinical Investigations, 2007.
Available
at:
http://www.fda.gov/OHRMS/
DOCKETS/98fr/04d-0440-gdl0002.pdf
Lu Z. Information Technology in Pharmaco
vigilance: Benefits, Challenges, and Future
Directions from Industry Perspectives. Drug,
Healthcare and Patient Safety. 2009;1:3545
Lu Z, Su J. Clinical Data Management: Current
Status, Challenges, and Future Directions from
Industry Perspectives. Open Access Journal of
Clinical Trials 2010; 2: 93-105
Walther B, Hossin S, Townend J, Abernethy N,
Parker D, Jeffries D. Comparison of Electronic
Data Capture (EDC) with the Standard Data
Capture. Method for Clinical Trial Data. PLoS
ONE.2011;6(9):25348
679
Rituraj et al.,
Int J Med Res Health Sci. 2015;4(3):675-679
You might also like
- Basics of Case Report Form Designing in Clinical ResearchDocument9 pagesBasics of Case Report Form Designing in Clinical ResearchEmilyMejiaNo ratings yet
- Basics of designing clinical case report formsDocument8 pagesBasics of designing clinical case report formsParthaNo ratings yet
- Basics of designing clinical case report formsDocument8 pagesBasics of designing clinical case report formsParthaNo ratings yet
- The DCT PlaybookDocument16 pagesThe DCT PlaybookDan Jecan100% (1)
- The Paper Trail: CRFS, Source Documents and Data Collection ToolsDocument5 pagesThe Paper Trail: CRFS, Source Documents and Data Collection ToolsSagaram ShashidarNo ratings yet
- Exploring The Progression of Electronic Data Capture (EDC) in Clinical TrialsDocument5 pagesExploring The Progression of Electronic Data Capture (EDC) in Clinical TrialsClinical ResearchNo ratings yet
- Introduction to Clinical Data ManagementDocument11 pagesIntroduction to Clinical Data ManagementPr Pa100% (1)
- Basics of CRF Design in Clinical ResearchDocument10 pagesBasics of CRF Design in Clinical ResearchDivyaNo ratings yet
- A1 AA 1 CPRS Usability SittigDocument17 pagesA1 AA 1 CPRS Usability SittigAiman AlrawabdehNo ratings yet
- Nursing TicsDocument22 pagesNursing TicssalatiitNo ratings yet
- EDCDocument40 pagesEDCNewlife MoveonNo ratings yet
- Evidence-Based Nursing Informatics, Quality and SafetyDocument36 pagesEvidence-Based Nursing Informatics, Quality and Safetymagdaashaaban100% (1)
- Computer Patient Record System: Lecaros, Langeras, Linaac, Llorente, Macapayad, Polistico, Pasion BSNB-2 NCM 110Document12 pagesComputer Patient Record System: Lecaros, Langeras, Linaac, Llorente, Macapayad, Polistico, Pasion BSNB-2 NCM 110Ashley Jane MacapayadNo ratings yet
- A Primer On Endoscopic Electronic Medical RecordsDocument6 pagesA Primer On Endoscopic Electronic Medical RecordsAceNo ratings yet
- HOSPITAL MANAGEMENT SYSTEMDocument30 pagesHOSPITAL MANAGEMENT SYSTEMDaniel braveNo ratings yet
- Major Oroject On Management Information SystemDocument48 pagesMajor Oroject On Management Information SystemAbhimanyuGulatiNo ratings yet
- ProposalDocument7 pagesProposalIlyasoft KP Peshawar100% (1)
- RFID Inventory Management SystemDocument4 pagesRFID Inventory Management SystemRaym MirandaNo ratings yet
- Research Paper EhrDocument4 pagesResearch Paper Ehrafeaxbgqp100% (3)
- Polytechnic University of The Philippines Electronics and Communications Engineering Automated Laboratory (Autolab) System For Transaction and Equipment MonitoringDocument8 pagesPolytechnic University of The Philippines Electronics and Communications Engineering Automated Laboratory (Autolab) System For Transaction and Equipment MonitoringesatjournalsNo ratings yet
- EHR AssignmentDocument7 pagesEHR AssignmentLisbon TsvarayiNo ratings yet
- Standard Operating Procedure (SOP) Research and Development OfficeDocument9 pagesStandard Operating Procedure (SOP) Research and Development OfficeTripti DuttaNo ratings yet
- COVID 19 With HospitalDocument41 pagesCOVID 19 With HospitalInitz TechnologiesNo ratings yet
- Data Collection For Research Source Documents and The Case Report Form (CRF)Document14 pagesData Collection For Research Source Documents and The Case Report Form (CRF)sprfyllisNo ratings yet
- JournalDocument11 pagesJournalNurullitaNo ratings yet
- Developing and Writing CRFDocument23 pagesDeveloping and Writing CRFsuri333No ratings yet
- Research Proposal ArushaDocument15 pagesResearch Proposal ArushaBONAVENTURE DEDENo ratings yet
- GNUmed Introduction v4Document14 pagesGNUmed Introduction v4trabajadosNo ratings yet
- A Computer-Based Patient Record For Improving Nursing CareDocument7 pagesA Computer-Based Patient Record For Improving Nursing CareBibiVmvNo ratings yet
- Maintaining Safety and Quality in Healthcare Through Information TechnologyDocument50 pagesMaintaining Safety and Quality in Healthcare Through Information TechnologymagdaashaabanNo ratings yet
- Hospital Management System ProjectDocument6 pagesHospital Management System ProjectAdjei JanetNo ratings yet
- Hospital Management SystemDocument17 pagesHospital Management SystemhyklassNo ratings yet
- ProjectDocument88 pagesProjectManash KumarNo ratings yet
- Data Management For Clinical Research - Home - CourseraDocument7 pagesData Management For Clinical Research - Home - Courseraashutosh0% (1)
- NG - 12911 243Document61 pagesNG - 12911 243emmanueljohnsonsmileNo ratings yet
- Ian Manzo Dental Appointment SystemDocument23 pagesIan Manzo Dental Appointment SystemRodel SisicanNo ratings yet
- Implementation of Electronic Data Capture Systems: Barriers and SolutionsDocument8 pagesImplementation of Electronic Data Capture Systems: Barriers and SolutionsKSatria BerGitarNo ratings yet
- E HealthDocument19 pagesE HealthAdeyemo RaphaelNo ratings yet
- Project Report On HOSPITAL ManagementDocument69 pagesProject Report On HOSPITAL ManagementAshwini Sowmya R100% (5)
- "Doctor-Patient Interaction System ": Kajol Kamble. Seat NO:-183440Document34 pages"Doctor-Patient Interaction System ": Kajol Kamble. Seat NO:-183440Poonam PawaleNo ratings yet
- The Study Protocol Part TwoDocument12 pagesThe Study Protocol Part TwoGerman LambogliaNo ratings yet
- Perceived Effectiveness of Clinical Pathway Soft 2020 International JournalDocument9 pagesPerceived Effectiveness of Clinical Pathway Soft 2020 International JournalxuebiduNo ratings yet
- BMC Medical Research MethodologyDocument25 pagesBMC Medical Research Methodologyhubik38No ratings yet
- Mini Project Report On Pathology Lab ManagementDocument53 pagesMini Project Report On Pathology Lab Managementkinuabha50% (2)
- Organ Sharing-Donator and Finder Using PHPDocument4 pagesOrgan Sharing-Donator and Finder Using PHPLogaNathanNo ratings yet
- Laboratory Data in EHRs 2014Document20 pagesLaboratory Data in EHRs 2014sairi_nagarajuNo ratings yet
- Design and Implementation of Appointment Management System (A CASE STUDY OF Federal Medical Center (FMC) .)Document52 pagesDesign and Implementation of Appointment Management System (A CASE STUDY OF Federal Medical Center (FMC) .)DAVIS ISIBOR100% (4)
- Ijamscr 19 359 - 915 920Document6 pagesIjamscr 19 359 - 915 920Azwar MudaNo ratings yet
- PMCF GuideDocument29 pagesPMCF GuideSandra SilvaNo ratings yet
- Visualization of CDA Laboratory Reports and Long Term Trends As A Possible EHR Application For Patients and PhysiciansDocument8 pagesVisualization of CDA Laboratory Reports and Long Term Trends As A Possible EHR Application For Patients and PhysiciansBora YüretNo ratings yet
- Final Year Project: Doctor Appointment Booking System: Project ID: FYP1-F19-E14Document26 pagesFinal Year Project: Doctor Appointment Booking System: Project ID: FYP1-F19-E14Arfan Chatha75% (4)
- Order 222Document7 pagesOrder 222Timothy OgomaNo ratings yet
- Hospital Management System ProjectDocument64 pagesHospital Management System ProjectrishabhmaithaniNo ratings yet
- B.1 Learning Objectives: System Life Cycle: at The End of The Lesson, The Student Should Be Able ToDocument73 pagesB.1 Learning Objectives: System Life Cycle: at The End of The Lesson, The Student Should Be Able ToPark Yoon AeNo ratings yet
- "Hospital Management System": Submited byDocument31 pages"Hospital Management System": Submited byNaveenNo ratings yet
- Hospital Management SystemDocument39 pagesHospital Management SystemMeenahNo ratings yet
- PACS EHR software proposal for Fortis HealthcareDocument12 pagesPACS EHR software proposal for Fortis HealthcareAmanpreet VaseerNo ratings yet
- Data Fusion Techniques and Applications for Smart HealthcareFrom EverandData Fusion Techniques and Applications for Smart HealthcareAmit Kumar SinghNo ratings yet
- Towards best practice in the Archetype Development ProcessFrom EverandTowards best practice in the Archetype Development ProcessNo ratings yet
- Ijmrhs Vol 4 Issue 4Document193 pagesIjmrhs Vol 4 Issue 4editorijmrhs0% (1)
- Ijmrhs Vol 4 Issue 3Document263 pagesIjmrhs Vol 4 Issue 3editorijmrhsNo ratings yet
- Ijmrhs Vol 4 Issue 2Document219 pagesIjmrhs Vol 4 Issue 2editorijmrhsNo ratings yet
- Ijmrhs Vol 2 Issue 3Document399 pagesIjmrhs Vol 2 Issue 3editorijmrhs100% (1)
- Ijmrhs Vol 1 Issue 1Document257 pagesIjmrhs Vol 1 Issue 1editorijmrhsNo ratings yet
- Ijmrhs Vol 1 Issue 1Document257 pagesIjmrhs Vol 1 Issue 1editorijmrhsNo ratings yet
- Ijmrhs Vol 3 Issue 4Document294 pagesIjmrhs Vol 3 Issue 4editorijmrhsNo ratings yet
- Ijmrhs Vol 2 Issue 4Document321 pagesIjmrhs Vol 2 Issue 4editorijmrhsNo ratings yet
- Ijmrhs Vol 3 Issue 3Document271 pagesIjmrhs Vol 3 Issue 3editorijmrhsNo ratings yet
- Ijmrhs Vol 3 Issue 2Document281 pagesIjmrhs Vol 3 Issue 2editorijmrhsNo ratings yet
- Ijmrhs Vol 3 Issue 1Document228 pagesIjmrhs Vol 3 Issue 1editorijmrhsNo ratings yet
- Ijmrhs Vol 2 Issue 2Document197 pagesIjmrhs Vol 2 Issue 2editorijmrhsNo ratings yet
- 43chaitali EtalDocument3 pages43chaitali EtaleditorijmrhsNo ratings yet
- 47serban Turliuc EtalDocument4 pages47serban Turliuc EtaleditorijmrhsNo ratings yet
- Ijmrhs Vol 2 Issue 1Document110 pagesIjmrhs Vol 2 Issue 1editorijmrhs100% (1)
- 36rashmipal EtalDocument6 pages36rashmipal EtaleditorijmrhsNo ratings yet
- 48 MakrandDocument2 pages48 MakrandeditorijmrhsNo ratings yet
- 38vaishnavi EtalDocument3 pages38vaishnavi EtaleditorijmrhsNo ratings yet
- Recurrent Cornual Ectopic Pregnancy - A Case Report: Article InfoDocument2 pagesRecurrent Cornual Ectopic Pregnancy - A Case Report: Article InfoeditorijmrhsNo ratings yet
- Williams-Campbell Syndrome-A Rare Entity of Congenital Bronchiectasis: A Case Report in AdultDocument3 pagesWilliams-Campbell Syndrome-A Rare Entity of Congenital Bronchiectasis: A Case Report in AdulteditorijmrhsNo ratings yet
- 45mohit EtalDocument4 pages45mohit EtaleditorijmrhsNo ratings yet
- 41anurag EtalDocument2 pages41anurag EtaleditorijmrhsNo ratings yet
- 37poflee EtalDocument3 pages37poflee EtaleditorijmrhsNo ratings yet
- 40vedant EtalDocument4 pages40vedant EtaleditorijmrhsNo ratings yet
- 34tupe EtalDocument5 pages34tupe EtaleditorijmrhsNo ratings yet
- Pernicious Anemia in Young: A Case Report With Review of LiteratureDocument5 pagesPernicious Anemia in Young: A Case Report With Review of LiteratureeditorijmrhsNo ratings yet
- 33 Prabu RamDocument5 pages33 Prabu RameditorijmrhsNo ratings yet
- 35krishnasamy EtalDocument1 page35krishnasamy EtaleditorijmrhsNo ratings yet
- 32bheemprasad EtalDocument3 pages32bheemprasad EtaleditorijmrhsNo ratings yet
- Abuse Prevention App - Research Paper (Engr. Madeeha Saeed)Document87 pagesAbuse Prevention App - Research Paper (Engr. Madeeha Saeed)Engr. Madeeha SaeedNo ratings yet
- Library Management System - ProposalDocument4 pagesLibrary Management System - ProposalIroshan Priyantha95% (43)
- Information Technology P1 Nov 2021 EngDocument25 pagesInformation Technology P1 Nov 2021 EngRue HartNo ratings yet
- DBMS Chapter 6 practice questions and answersDocument6 pagesDBMS Chapter 6 practice questions and answersThanusri. SNo ratings yet
- Travel Agency Software - DocumentationDocument42 pagesTravel Agency Software - DocumentationMadeleine Sangoi100% (1)
- Er ModelDocument69 pagesEr Modelgayathri cseNo ratings yet
- Test Bank For Modern Database Management 11 e 11th Edition Jeffrey A Hoffer V Ramesh Heikki TopiDocument25 pagesTest Bank For Modern Database Management 11 e 11th Edition Jeffrey A Hoffer V Ramesh Heikki TopiMaryJohnsonafrz100% (43)
- MySQL NotesDocument58 pagesMySQL NotesPrecious WaseniNo ratings yet
- Bridge Management Systems: Literature ReviewDocument3 pagesBridge Management Systems: Literature ReviewNiroshan KarunarathnaNo ratings yet
- OOAD Record NewDocument133 pagesOOAD Record Newnandhakumar.pornstarNo ratings yet
- Conceptual Modeling and Entity-Relationship Diagrams: Chapter 3: Elmasri/NavatheDocument52 pagesConceptual Modeling and Entity-Relationship Diagrams: Chapter 3: Elmasri/NavatheHARDIK PANPALIYANo ratings yet
- Exchange 2003 Backup Restore & RecoveryDocument64 pagesExchange 2003 Backup Restore & RecoveryRajeev KumarNo ratings yet
- Sap Bods TutorialDocument26 pagesSap Bods TutorialPavan Sandeep V V0% (1)
- Portal TroubleshootDocument145 pagesPortal Troubleshootdcoll1isNo ratings yet
- 2020-21 M.C.A. (Affiliated Colleges and Instituite)Document58 pages2020-21 M.C.A. (Affiliated Colleges and Instituite)Brothers CreationNo ratings yet
- SAP R3 Client Server ArchitectureDocument4 pagesSAP R3 Client Server ArchitecturePrerna KakkarNo ratings yet
- Data Journalism BookDocument48 pagesData Journalism BookJelena RodicNo ratings yet
- It Sba 2021Document7 pagesIt Sba 2021Peta-Kay TuckerNo ratings yet
- MIS Assignment - I: Answer-1Document8 pagesMIS Assignment - I: Answer-1krati jainNo ratings yet
- Test Bank For Database Processing: Fundamentals, Design, and Implementation, 13/E 13th Edition David M. Kroenke, David J. AuerDocument36 pagesTest Bank For Database Processing: Fundamentals, Design, and Implementation, 13/E 13th Edition David M. Kroenke, David J. Aueramyharveyqznmbipkyr100% (13)
- Function Specifications in SAPDocument6 pagesFunction Specifications in SAPRamesh BalajiNo ratings yet
- Plan GDocument11 pagesPlan Gbelly7308No ratings yet
- Computer Aided Process Planning (CAPP)Document30 pagesComputer Aided Process Planning (CAPP)brijkishor2017100% (1)
- Igcse Ict GlossaryDocument0 pagesIgcse Ict GlossaryChyrsella Verena100% (2)
- Sales Operations Manager ResumeDocument1 pageSales Operations Manager Resumerothko75No ratings yet
- DWH Fundamentals (Training Material)Document21 pagesDWH Fundamentals (Training Material)svdonthaNo ratings yet
- ManegemeneDocument26 pagesManegemeneTk ChichieNo ratings yet
- Student Academic History 6.1 012704Document51 pagesStudent Academic History 6.1 012704Jair EstradaNo ratings yet
- Foundation of Quality ManagementDocument19 pagesFoundation of Quality ManagementAmit VijayvargiyaNo ratings yet
- "Student Management System": A Project Report ONDocument10 pages"Student Management System": A Project Report ONRishav BansalNo ratings yet