You might also like
- Oral Wound Healing: Cell Biology and Clinical ManagementFrom EverandOral Wound Healing: Cell Biology and Clinical ManagementHannu LarjavaNo ratings yet
- Sample Questions MJDF Part 1 Sample Questions MJDF Part 1Document21 pagesSample Questions MJDF Part 1 Sample Questions MJDF Part 1HarkanNo ratings yet
- Changing Concepts in Cariology - Forty Years OnDocument7 pagesChanging Concepts in Cariology - Forty Years OnDavid CaminoNo ratings yet
- Lecture 5 Laser in Operative DentistryDocument7 pagesLecture 5 Laser in Operative DentistryDt omarNo ratings yet
- Failures in Periodontal Therapy: Review ArticleDocument6 pagesFailures in Periodontal Therapy: Review ArticlezinniaNo ratings yet
- ProposalDocument5 pagesProposalapi-354921474No ratings yet
- Dental AuxiliariesDocument14 pagesDental AuxiliariesnainaNo ratings yet
- Immunology Dental Caries-2015Document24 pagesImmunology Dental Caries-2015Bagus Rahmawan50% (2)
- Lecture 4 Diagnosis of Dental CariesDocument12 pagesLecture 4 Diagnosis of Dental CariesDt omarNo ratings yet
- Orofacial Infections in Children PedoDocument40 pagesOrofacial Infections in Children PedoFourthMolar.comNo ratings yet
- Interpretation of OpgDocument6 pagesInterpretation of Opgjawaad29375% (8)
- Pediatric Dentistry Exam QuestionnaireDocument2 pagesPediatric Dentistry Exam QuestionnaireVagelis RaftopoulosNo ratings yet
- Endodontic Failures-A Review: Dr. Sadashiv Daokar, DR - Anita.KalekarDocument6 pagesEndodontic Failures-A Review: Dr. Sadashiv Daokar, DR - Anita.KalekarGunjan GargNo ratings yet
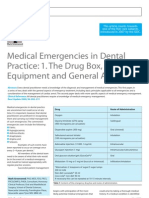
- Medical Emergencies in Dental Practice: 1. The Drug Box, Equipment and General ApproachDocument6 pagesMedical Emergencies in Dental Practice: 1. The Drug Box, Equipment and General ApproachRodelix San Juan Dacanay100% (1)
- Articaine Dental Update 2015Document5 pagesArticaine Dental Update 2015Ashley WrightNo ratings yet
- MJDF Part 1 QuestionsDocument21 pagesMJDF Part 1 QuestionsHabeeb AL-AbsiNo ratings yet
- Classification of Dental CariesDocument80 pagesClassification of Dental CariesOsman SoormaNo ratings yet
- Rationale of Periodontal TreatmentDocument5 pagesRationale of Periodontal Treatmentdileep9002392No ratings yet
- Oral Diagnosis and Treatment Planning: Part 7. Treatment Planning For Missing TeethDocument11 pagesOral Diagnosis and Treatment Planning: Part 7. Treatment Planning For Missing TeethalfredoibcNo ratings yet
- Periodontal Therapy StatementDocument7 pagesPeriodontal Therapy StatementDiana AlexandraNo ratings yet
- Oral and Maxillofacial SurgeryDocument6 pagesOral and Maxillofacial Surgerysunaina chopraNo ratings yet
- Vertical Root Fracture !Document42 pagesVertical Root Fracture !Dr Dithy kkNo ratings yet
- MGR Univ - PerioDocument8 pagesMGR Univ - PerioMohamed FaizalNo ratings yet
- Dentosphere - World of Dentistry - MCQs in Endodontics - Disinfection and ObturationDocument14 pagesDentosphere - World of Dentistry - MCQs in Endodontics - Disinfection and Obturationbadr abdelkaderNo ratings yet
- Avulsion: DEFINITION: - Tooth Avulsion (Exarticulation) Implies Total Displacement of The ToothDocument39 pagesAvulsion: DEFINITION: - Tooth Avulsion (Exarticulation) Implies Total Displacement of The Toothshailesh_shenoyNo ratings yet
- Emergency Drugs in Dental PracticeDocument3 pagesEmergency Drugs in Dental PracticeRishwan Omer SalihNo ratings yet
- A 100-Year Journey From GV Black To Minimal Surgical InterventionDocument6 pagesA 100-Year Journey From GV Black To Minimal Surgical InterventionMichael XuNo ratings yet
- Antibiotic Prophylaxis in DentistryDocument9 pagesAntibiotic Prophylaxis in DentistryLiana OpriţăNo ratings yet
- MDS Oral Medicine Question Papers 2002Document5 pagesMDS Oral Medicine Question Papers 2002Niyas UmmerNo ratings yet
- Reducing The Risk of Failure Incomplete Denture PatientsDocument8 pagesReducing The Risk of Failure Incomplete Denture PatientsHisyam IshakNo ratings yet
- 5 PDFDocument8 pages5 PDFoskar ORTIZNo ratings yet
- Dental Considerations-CVS DiseasesDocument86 pagesDental Considerations-CVS Diseasesapi-3704106100% (1)
- 11-Impacted Third MolarDocument117 pages11-Impacted Third MolarAhmed aljumailiNo ratings yet
- 2015Document45 pages2015jimmyNo ratings yet
- Chapter 2: Operative Dentistry and Prosthodontics: AnswersDocument13 pagesChapter 2: Operative Dentistry and Prosthodontics: AnswersBinayak UpadhyayaNo ratings yet
- Department of Pedodontics: Submitted By: Shayoni Sen Bds Ivth YearDocument29 pagesDepartment of Pedodontics: Submitted By: Shayoni Sen Bds Ivth YearFarzana ShereenNo ratings yet
- Endomishaps SeminarDocument44 pagesEndomishaps SeminarSuma TettaNo ratings yet
- Krok 2 Stomatology: Test Items For Licensing ExaminationDocument30 pagesKrok 2 Stomatology: Test Items For Licensing ExaminationjimmyNo ratings yet
- Vital Therapy in Carious ToothDocument9 pagesVital Therapy in Carious ToothAsh PeiNo ratings yet
- 2020 Tongue Disorders Ods 210Document25 pages2020 Tongue Disorders Ods 210Farhaana ShaboodienNo ratings yet
- Tips On Access Cavity Preparation.: How To' TechniqueDocument4 pagesTips On Access Cavity Preparation.: How To' TechniqueGoran TosicNo ratings yet
- MCQs On Oral Histology - Dental Pulp - 1-5Document5 pagesMCQs On Oral Histology - Dental Pulp - 1-5Karizma TravelNo ratings yet
- Australian Dental Journal: Rhinosinusitis in Oral Medicine and DentistryDocument7 pagesAustralian Dental Journal: Rhinosinusitis in Oral Medicine and DentistryVishakha SabooNo ratings yet
- Literature GuideDocument60 pagesLiterature Guide12345sagarNo ratings yet
- 5-Plaque and CalculusDocument174 pages5-Plaque and CalculusAJPEDO LIFE100% (1)
- Medical Engineering & PhysicsDocument6 pagesMedical Engineering & PhysicsLuis Fernando Guayllas PomaNo ratings yet
- Caldwell TechniqueDocument4 pagesCaldwell TechniqueNurul RamadhantyNo ratings yet
- GingivectomyDocument5 pagesGingivectomyRomzi HanifNo ratings yet
- Dental Plaque: By:-Raina J. P. Khanam Post Graduate 2 Year Dept. of Periodontics and ImplantologyDocument69 pagesDental Plaque: By:-Raina J. P. Khanam Post Graduate 2 Year Dept. of Periodontics and ImplantologyAtul KoundelNo ratings yet
- Cavity design techniques for optimizing Class IV composite restorationsDocument6 pagesCavity design techniques for optimizing Class IV composite restorationselokfaiqNo ratings yet
- Role of A Pedodontist in Cleft Lip and Cleft Palate Rehabilitation - An OverviewDocument25 pagesRole of A Pedodontist in Cleft Lip and Cleft Palate Rehabilitation - An OverviewIJAR JOURNALNo ratings yet
- 31 SJ BDJ 2014 953Document7 pages31 SJ BDJ 2014 953Juan Augusto Fernández TarazonaNo ratings yet
- INBDE Item - Development - Guide - Appendices - A-EDocument95 pagesINBDE Item - Development - Guide - Appendices - A-ESharjeel ChaudhryNo ratings yet
- CG A021 01 Comprehensive Oral ExaminationDocument13 pagesCG A021 01 Comprehensive Oral Examinationmahmoud100% (1)
- Abnormalities of Teeth1.2020Document5 pagesAbnormalities of Teeth1.2020Farhaana ShaboodienNo ratings yet
- 03 MFDS Regulations & Syllabus 2011Document15 pages03 MFDS Regulations & Syllabus 2011FarahMohammed1No ratings yet
- 3D Printing in Periodontics A ReviewDocument11 pages3D Printing in Periodontics A ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- DENTAL AUXILIARY EDUCATION EXAMINATION IN DENTAL MATERIALS: Passbooks Study GuideFrom EverandDENTAL AUXILIARY EDUCATION EXAMINATION IN DENTAL MATERIALS: Passbooks Study GuideNo ratings yet
- AnatomyDocument91 pagesAnatomysarahNo ratings yet
- Physiology MCQDocument3 pagesPhysiology MCQDr Md Abedur Rahman90% (10)
- When To Plan PFM ExtractionsDocument10 pagesWhen To Plan PFM ExtractionssarahNo ratings yet
- Denture BaseDocument59 pagesDenture BasesarahNo ratings yet
- Partial Removable Dental Prosthesis GuideDocument37 pagesPartial Removable Dental Prosthesis Guidesarah0% (1)
- Physiology MCQDocument3 pagesPhysiology MCQDr Md Abedur Rahman90% (10)
- Oral Histology MCQsDocument27 pagesOral Histology MCQssarah100% (2)
- Bone Tumors HODocument81 pagesBone Tumors HOOsman SoormaNo ratings yet
- Abnormalities of Primary and Mixed DentitionDocument39 pagesAbnormalities of Primary and Mixed DentitionsarahNo ratings yet
- Relining in RPD!Document33 pagesRelining in RPD!sarah50% (2)
- Denture BaseDocument59 pagesDenture BasesarahNo ratings yet
- 1-Impression TechniquesTheoriesDocument19 pages1-Impression TechniquesTheoriessarahNo ratings yet
- Management of Maxillofacial TraumaDocument33 pagesManagement of Maxillofacial TraumaAdilah Afifah67% (6)
- Thyroid Cancer: Causes, Types, Diagnosis and TreatmentDocument38 pagesThyroid Cancer: Causes, Types, Diagnosis and TreatmentsarahNo ratings yet
- Minor ConnectorsDocument61 pagesMinor Connectorssarah100% (1)
- Treatment Plan For Periodontal Diseases NEWDocument20 pagesTreatment Plan For Periodontal Diseases NEWsarahNo ratings yet
- Indirect RetainersDocument52 pagesIndirect RetainerssarahNo ratings yet
- Indirect RetainersDocument52 pagesIndirect RetainerssarahNo ratings yet
- Thyroid Cancer: Causes, Types, Diagnosis and TreatmentDocument38 pagesThyroid Cancer: Causes, Types, Diagnosis and TreatmentsarahNo ratings yet
- ENT Lecture!Document31 pagesENT Lecture!sarahNo ratings yet
- Cleft Lip PalateDocument35 pagesCleft Lip PalatesarahNo ratings yet
- Jaw DisorderDocument42 pagesJaw DisordersarahNo ratings yet
- Odontomes and Odontogenic TumoursDocument16 pagesOdontomes and Odontogenic TumourssarahNo ratings yet
- Periodontal PocketDocument31 pagesPeriodontal Pocketperiodontics07No ratings yet
- Thyroid Cancer: Causes, Types, Diagnosis and TreatmentDocument38 pagesThyroid Cancer: Causes, Types, Diagnosis and TreatmentsarahNo ratings yet
- Oral Medicine Exam QuestionsDocument8 pagesOral Medicine Exam QuestionssarahNo ratings yet
- Aarish Billing SheetDocument6 pagesAarish Billing SheetSatish VirasNo ratings yet
- Woman With DysuriaDocument26 pagesWoman With DysuriaAlFi KamaliaNo ratings yet
- Nursing PhilosophyDocument6 pagesNursing Philosophyapi-541532244No ratings yet
- DISCHARGE MEDICATIONS AND INSTRUCTIONSDocument1 pageDISCHARGE MEDICATIONS AND INSTRUCTIONSJOHN PEARL FERNANDEZNo ratings yet
- Medicina Natural GatosDocument40 pagesMedicina Natural GatosfdfdfdfNo ratings yet
- A Review On Netra Tarpana - An Ayurveda Method of Eye Care: January 2021Document10 pagesA Review On Netra Tarpana - An Ayurveda Method of Eye Care: January 2021Lepaksha GowdaNo ratings yet
- Understanding Clinical Trials - PDDocument7 pagesUnderstanding Clinical Trials - PDCristina SalcianuNo ratings yet
- Core Components-Competence NursingDocument2 pagesCore Components-Competence NursingitunuNo ratings yet
- Usmle Step 1 Experience Omar AkramDocument6 pagesUsmle Step 1 Experience Omar AkramAbdirahmanNo ratings yet
- Nursing Procedure Checklist: Administering Oral MedicationsDocument2 pagesNursing Procedure Checklist: Administering Oral MedicationsOrl Trinidad100% (1)
- Pathology Lecture 7 - LiverDocument11 pagesPathology Lecture 7 - Livercgao30No ratings yet
- Presentation Grouping With TopicsDocument10 pagesPresentation Grouping With TopicsEnnara VellaniNo ratings yet
- 2022 Springer Nature Fully Open Access JournalsDocument36 pages2022 Springer Nature Fully Open Access JournalsEntertainment HubNo ratings yet
- (Makalah) Implementasi Aplikasi CPD Online Dalam Mendukung E-STR Versi 2.0 PDFDocument155 pages(Makalah) Implementasi Aplikasi CPD Online Dalam Mendukung E-STR Versi 2.0 PDFAmelia PuspitaNo ratings yet
- Nursing Care Plan Breast Feeding IneffectiveDocument1 pageNursing Care Plan Breast Feeding Ineffectivederic88% (8)
- Diagnosis of TuberculosisDocument5 pagesDiagnosis of TuberculosisahmedNo ratings yet
- Unit 2A - Course NotesDocument162 pagesUnit 2A - Course Notesrashid zaman100% (5)
- Chapter 29: Multiple Choice Questions: InstructionsDocument2 pagesChapter 29: Multiple Choice Questions: InstructionsLola Muhoza100% (1)
- Oral Ulcerative Lesions 1 PDFDocument33 pagesOral Ulcerative Lesions 1 PDFUmmu MujahidahNo ratings yet
- Ebp Presentation 1Document21 pagesEbp Presentation 1api-340248301No ratings yet
- Food and Fertility: What Should Women Consume When Trying To Conceive?Document2 pagesFood and Fertility: What Should Women Consume When Trying To Conceive?Gerry FonziNo ratings yet
- PromixineDocument2 pagesPromixineStelaA1No ratings yet
- Health & Safety Leaflet UpdatedDocument3 pagesHealth & Safety Leaflet UpdatedMicheal McDowellNo ratings yet
- Family Nursing Care PlanDocument4 pagesFamily Nursing Care PlanJamaica Mae AguilarNo ratings yet
- MSDs in The WorkplaceDocument403 pagesMSDs in The WorkplaceAden ParkerNo ratings yet
- Major Stakeholders in Health Care SystemDocument5 pagesMajor Stakeholders in Health Care SystemANITTA S100% (1)
- 12th Grade Veisalgia Text - QuestionsDocument3 pages12th Grade Veisalgia Text - QuestionsNUJMATUL HUDA AHARUL HADAFINo ratings yet
- Pediatric EmergencyDocument1 pagePediatric EmergencycilengsaiNo ratings yet
- BCG Vaccine: Serum Institute of India Pvt. LTDDocument1 pageBCG Vaccine: Serum Institute of India Pvt. LTDkemalahmadNo ratings yet
- Latihan Pareto ChartDocument4 pagesLatihan Pareto ChartkasmawatiNo ratings yet