You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Covid 19 CPR 7 RulesDocument21 pagesCovid 19 CPR 7 RulesMiguel Cuevas DolotNo ratings yet
- Cook Book (Filipino) 13 PDFDocument23 pagesCook Book (Filipino) 13 PDFAdina AnghelNo ratings yet
- Covid 19 CPR 7 RulesDocument21 pagesCovid 19 CPR 7 RulesMiguel Cuevas DolotNo ratings yet
- PSB 368Document6 pagesPSB 368Miguel Cuevas DolotNo ratings yet
- Benign Paroxysmal Positional Vertigo: Waseem WatadDocument37 pagesBenign Paroxysmal Positional Vertigo: Waseem WatadnoviNo ratings yet
- Vertigo Gail Ishiyama 1 13 10Document40 pagesVertigo Gail Ishiyama 1 13 10Myname Rama LienNo ratings yet
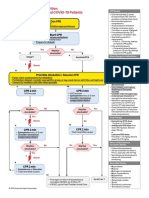
- ACLS Cardiac Arrest Algorithm For Suspected or Confirmed COVID-19 PatientsDocument1 pageACLS Cardiac Arrest Algorithm For Suspected or Confirmed COVID-19 PatientsMariuxi Tatiana ChocoNo ratings yet
- Effectiveness of Transdermal MagnesiumDocument2 pagesEffectiveness of Transdermal MagnesiumMiguel Cuevas Dolot100% (1)
- How Can Patients Visitors Help - May18Document2 pagesHow Can Patients Visitors Help - May18Miguel Cuevas DolotNo ratings yet
- Physical Examination in ENT: Ussana Promyothin, MDDocument60 pagesPhysical Examination in ENT: Ussana Promyothin, MDMiguel Cuevas DolotNo ratings yet
- Clinical Examination of The Ear, Nose and Throat: Dave Pothier ST Mary's 2003Document30 pagesClinical Examination of The Ear, Nose and Throat: Dave Pothier ST Mary's 2003Ekambaram TrmNo ratings yet
- Active Listening HANDOUT PDFDocument26 pagesActive Listening HANDOUT PDFMiguel Cuevas DolotNo ratings yet
- (MED) COVID-19 Trans V. 2.0Document6 pages(MED) COVID-19 Trans V. 2.0Isabel VinasNo ratings yet
- Physical Examination in ENT: Ussana Promyothin, MDDocument60 pagesPhysical Examination in ENT: Ussana Promyothin, MDMiguel Cuevas DolotNo ratings yet
- Physical Assessment: Ear, Nose, Mouth, and ThroatDocument59 pagesPhysical Assessment: Ear, Nose, Mouth, and ThroatMiguel Cuevas DolotNo ratings yet
- Covid 19 PDFDocument18 pagesCovid 19 PDFMiguel Cuevas DolotNo ratings yet
- Clinical AbstractDocument4 pagesClinical AbstractMiguel Cuevas DolotNo ratings yet
- Pedia Tickler Update 2017Document2 pagesPedia Tickler Update 2017Tani BokNo ratings yet
- Neurologic ExamDocument1 pageNeurologic ExamMiguel Cuevas DolotNo ratings yet
- Drug IndexDocument2 pagesDrug IndexMiguel Cuevas DolotNo ratings yet
- A Case-Control Study of The Association of Diet and Obesity With Gout in Taiwan PDFDocument12 pagesA Case-Control Study of The Association of Diet and Obesity With Gout in Taiwan PDFMiguel Cuevas DolotNo ratings yet
- A Case-Control Study of The Association of Diet and Obesity With Gout in Taiwan PDFDocument12 pagesA Case-Control Study of The Association of Diet and Obesity With Gout in Taiwan PDFMiguel Cuevas DolotNo ratings yet
- Nocturnals Physiology 2018Document14 pagesNocturnals Physiology 2018Miguel Cuevas DolotNo ratings yet
- HEMAreviewDocument3 pagesHEMAreviewMiguel Cuevas DolotNo ratings yet
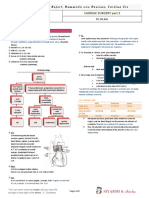
- TCVS - Cardiac Surgery Part 2 Dr. de AsisDocument8 pagesTCVS - Cardiac Surgery Part 2 Dr. de AsisMiguel Cuevas DolotNo ratings yet
- Anesthesia Pocket Cards 7 18 18Document6 pagesAnesthesia Pocket Cards 7 18 18Miguel Cuevas DolotNo ratings yet
- Pediatric History and Physical Exam GuideDocument7 pagesPediatric History and Physical Exam GuideIndunil AnuruddhikaNo ratings yet
- Community-Acquired Pneumonia - CPG 2016Document26 pagesCommunity-Acquired Pneumonia - CPG 2016Jamie SebastianNo ratings yet
- Kerosene PDFDocument31 pagesKerosene PDFRudyMLanaNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Eng10 LPQ3_4 Coherence and CohesionDocument2 pagesEng10 LPQ3_4 Coherence and CohesionNiña RasonableNo ratings yet
- Cast Copper Alloy Solder Joint Pressure Fittings: ASME B16.18-2018Document41 pagesCast Copper Alloy Solder Joint Pressure Fittings: ASME B16.18-2018crescon designNo ratings yet
- Journal of Electronic MaterialsDocument10 pagesJournal of Electronic MaterialsSanjib BaglariNo ratings yet
- Present Tense Exercises. Polish A1Document6 pagesPresent Tense Exercises. Polish A1Pilar Moreno DíezNo ratings yet
- HiaceDocument1 pageHiaceburjmalabarautoNo ratings yet
- A Model For Blockchain-Based Distributed Electronic Health Records - 2016Document14 pagesA Model For Blockchain-Based Distributed Electronic Health Records - 2016Asif KhalidNo ratings yet
- A Random-Walk-Down-Wall-Street-Malkiel-En-2834 PDFDocument5 pagesA Random-Walk-Down-Wall-Street-Malkiel-En-2834 PDFTim100% (1)
- Ferret Fiasco: Archie Carr IIIDocument8 pagesFerret Fiasco: Archie Carr IIIArchie Carr III100% (1)
- Class Homework Chapter 1Document9 pagesClass Homework Chapter 1Ela BallıoğluNo ratings yet
- Fright ForwordersDocument6 pagesFright ForworderskrishnadaskotaNo ratings yet
- New Member OrientationDocument41 pagesNew Member OrientationM.NASIRNo ratings yet
- 04 - JTC Template On Project ProposalDocument10 pages04 - JTC Template On Project Proposalbakelm alqamisNo ratings yet
- TOTAL Income: POSSTORE JERTEH - Account For 2021 Start Date 8/1/2021 End Date 8/31/2021Document9 pagesTOTAL Income: POSSTORE JERTEH - Account For 2021 Start Date 8/1/2021 End Date 8/31/2021Alice NguNo ratings yet
- Student Worksheet 8BDocument8 pagesStudent Worksheet 8BLatomeNo ratings yet
- Glowing Stones in Ancient LoreDocument16 pagesGlowing Stones in Ancient LorerippvannNo ratings yet
- SuccessDocument146 pagesSuccessscribdNo ratings yet
- KAMAGONGDocument2 pagesKAMAGONGjeric plumosNo ratings yet
- Engaged Listening Worksheet 3 - 24Document3 pagesEngaged Listening Worksheet 3 - 24John BennettNo ratings yet
- Fundamentals of Analytics in Practice /TITLEDocument43 pagesFundamentals of Analytics in Practice /TITLEAcad ProgrammerNo ratings yet
- Sikkim Public Works Liability of Government and Contractor Act 1983Document11 pagesSikkim Public Works Liability of Government and Contractor Act 1983Latest Laws TeamNo ratings yet
- The Apostolic Church, Ghana English Assembly - Koforidua District Topic: Equipping The Saints For The MinistryDocument2 pagesThe Apostolic Church, Ghana English Assembly - Koforidua District Topic: Equipping The Saints For The MinistryOfosu AnimNo ratings yet
- Calvo, G (1988) - Servicing The Public Debt - The Role of ExpectationsDocument16 pagesCalvo, G (1988) - Servicing The Public Debt - The Role of ExpectationsDaniela SanabriaNo ratings yet
- Marcos & Sumulong Highway, Rizal Applicant'S Information Sheet (Non-Academic)Document2 pagesMarcos & Sumulong Highway, Rizal Applicant'S Information Sheet (Non-Academic)dummy testerNo ratings yet
- Issues and Concerns Related To Assessment in MalaysianDocument22 pagesIssues and Concerns Related To Assessment in MalaysianHarrish ZainurinNo ratings yet
- Teaching Islamic Traditions by SlidesgoDocument48 pagesTeaching Islamic Traditions by SlidesgoCallista Naira AzkiaNo ratings yet
- Military Divers ManualDocument30 pagesMilitary Divers ManualJohn0% (1)
- Fitting A Logistic Curve To DataDocument12 pagesFitting A Logistic Curve To DataXiaoyan ZouNo ratings yet
- Keyboard notes to Fur Elise melodyDocument2 pagesKeyboard notes to Fur Elise melodyReji SarsalejoNo ratings yet
- Postmodern Dystopian Fiction: An Analysis of Bradbury's Fahrenheit 451' Maria AnwarDocument4 pagesPostmodern Dystopian Fiction: An Analysis of Bradbury's Fahrenheit 451' Maria AnwarAbdennour MaafaNo ratings yet
- Segmenting, Targeting, and Positioning (STP)Document16 pagesSegmenting, Targeting, and Positioning (STP)Rachmat PutraNo ratings yet