You might also like
- D2.8 New Challenges and New Methods For Outbreak Communication-Summary ReportDocument37 pagesD2.8 New Challenges and New Methods For Outbreak Communication-Summary ReportZadig srlNo ratings yet
- 14 Metodi LongDocument1 page14 Metodi LongZadig srlNo ratings yet
- ICT Key Enabling Technologies at The Service of European Citizens and CitiesDocument8 pagesICT Key Enabling Technologies at The Service of European Citizens and CitiesZadig srlNo ratings yet
- Integrated Assesments Models For Air PollutionsDocument82 pagesIntegrated Assesments Models For Air PollutionsZadig srlNo ratings yet
- Impact Assessment of Urban Green SpacesDocument25 pagesImpact Assessment of Urban Green SpacesZadig srlNo ratings yet
- The Future of ScienceDocument4 pagesThe Future of ScienceZadig srlNo ratings yet
- New Clinical Trial RegulationDocument2 pagesNew Clinical Trial RegulationZadig srlNo ratings yet
- Integrated Assesments Models For Air PollutionsDocument82 pagesIntegrated Assesments Models For Air PollutionsZadig srlNo ratings yet
- Environmental Impact Assessment of Ultra Fine Particles. Rome Case StudyDocument20 pagesEnvironmental Impact Assessment of Ultra Fine Particles. Rome Case StudyZadig srlNo ratings yet
- D3.1 New Framework Model For Outbreak CommunicationDocument23 pagesD3.1 New Framework Model For Outbreak CommunicationZadig srlNo ratings yet
- Air Pollution Modelling: An OverviewDocument57 pagesAir Pollution Modelling: An OverviewZadig srlNo ratings yet
- TELL ME D4.2 Software DesignDocument39 pagesTELL ME D4.2 Software DesignZadig srlNo ratings yet
- Air Pollution Modelling: An OverviewDocument57 pagesAir Pollution Modelling: An OverviewZadig srlNo ratings yet
- ECRAN - ICTD Meeting Program & InfoDocument8 pagesECRAN - ICTD Meeting Program & InfoZadig srlNo ratings yet
- EEA-Report 9-2013 Air-Quality in EuropeDocument112 pagesEEA-Report 9-2013 Air-Quality in EuropeVlad AndriescuNo ratings yet
- ECRAN - ICTD Meeting Program & InfoDocument8 pagesECRAN - ICTD Meeting Program & InfoZadig srlNo ratings yet
- D4 1 Architecture Technical Specifications and Validation CriteriaDocument16 pagesD4 1 Architecture Technical Specifications and Validation CriteriaZadig srlNo ratings yet
- Health Impact Assesment of Air Pollution (M.martuzzi Et Al.)Document6 pagesHealth Impact Assesment of Air Pollution (M.martuzzi Et Al.)Zadig srlNo ratings yet
- Imaging The Immune SystemDocument2 pagesImaging The Immune SystemZadig srlNo ratings yet
- Vaccini Come Paradigma Di Ricerca Al Servizio Della Salute GlobaleDocument38 pagesVaccini Come Paradigma Di Ricerca Al Servizio Della Salute GlobaleZadig srlNo ratings yet
- Locandina VII Annual Ri - MED Scientific Symposium PDFDocument1 pageLocandina VII Annual Ri - MED Scientific Symposium PDFZadig srlNo ratings yet
- Conflict Workshop Program PDFDocument5 pagesConflict Workshop Program PDFZadig srlNo ratings yet
- E96762 Final PDFDocument33 pagesE96762 Final PDFBalan PalaniappanNo ratings yet
- Advances in Environmental Epidemiology and Health Impact AssesmentDocument1 pageAdvances in Environmental Epidemiology and Health Impact AssesmentZadig srlNo ratings yet
- Locandina Prof James K. Galbraith PDFDocument1 pageLocandina Prof James K. Galbraith PDFZadig srlNo ratings yet
- WHO - Health Impact of PM10 and Ozone in 13 Italian CitiesDocument147 pagesWHO - Health Impact of PM10 and Ozone in 13 Italian CitiesZadig srlNo ratings yet
- FWD: (Climalt.) Editoriale Di Nature Climate ChangeDocument1 pageFWD: (Climalt.) Editoriale Di Nature Climate ChangeZadig srlNo ratings yet
- Scientific Data SharingDocument1 pageScientific Data SharingZadig srlNo ratings yet
- FiMat 2013Document42 pagesFiMat 2013Zadig srlNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5782)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- M1 Seminar Report 1Document26 pagesM1 Seminar Report 1naithivka rsNo ratings yet
- Review Materials: Prepared By: Junior Philippine Institute of Accountants UC-Banilad Chapter F.Y. 2019-2020Document19 pagesReview Materials: Prepared By: Junior Philippine Institute of Accountants UC-Banilad Chapter F.Y. 2019-2020AB CloydNo ratings yet
- Role and Functions of Beneficial Microorganisms in Sustainable AquacultureDocument7 pagesRole and Functions of Beneficial Microorganisms in Sustainable Aquaculturepig_pink1989No ratings yet
- The Five Kingdoms: Natural Science 2. Secondary EducationDocument10 pagesThe Five Kingdoms: Natural Science 2. Secondary Educationrizza cayabyabNo ratings yet
- Anther Pollen CultureDocument28 pagesAnther Pollen CultureSachin MauryaNo ratings yet
- Chapter 3 Nec OrganizationDocument1 pageChapter 3 Nec OrganizationMomtaz MoniNo ratings yet
- Hydraulic Design of Storm Sewers With Excel CourseDocument41 pagesHydraulic Design of Storm Sewers With Excel CourseRonal Salvatierra100% (1)
- Reports On How The CovidDocument2 pagesReports On How The CovidRama KanthNo ratings yet
- Ncma219 Course Task 4Document3 pagesNcma219 Course Task 4NikoruNo ratings yet
- Estimation of Fire Loads For An Educational Building - A Case StudyDocument4 pagesEstimation of Fire Loads For An Educational Building - A Case StudyEditor IJSETNo ratings yet
- Avi Volunteer GuidebookDocument44 pagesAvi Volunteer GuidebookReuben Henry HartNo ratings yet
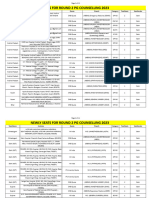
- Newly Seats For Round 2 PG Counselling 2023Document11 pagesNewly Seats For Round 2 PG Counselling 2023Manoj KumarNo ratings yet
- K85001-0646 - Intelligent Smoke DetectorDocument4 pagesK85001-0646 - Intelligent Smoke Detectorafie pio pioNo ratings yet
- Riverview Annual Report 2012Document4 pagesRiverview Annual Report 2012api-198623878No ratings yet
- Al Ansari Profile OmanDocument24 pagesAl Ansari Profile OmanMohamed RusfanNo ratings yet
- En - Product Catalogue Sniffin Sticks Rev5 - 43Document13 pagesEn - Product Catalogue Sniffin Sticks Rev5 - 43Elton MatsushimaNo ratings yet
- H Calculations - Enthalpy of SolutionDocument3 pagesH Calculations - Enthalpy of SolutionArif PurwadanaNo ratings yet
- OTHM All Course Flyer With Prices - 1Document5 pagesOTHM All Course Flyer With Prices - 1Ajun FranklinNo ratings yet
- Design Optimization of Ice Plant Test-Rig: H. S. Salave, V. N. RaibholeDocument6 pagesDesign Optimization of Ice Plant Test-Rig: H. S. Salave, V. N. RaibholeNeeraj SamadhiyaNo ratings yet
- United States Court of Appeals, Third CircuitDocument22 pagesUnited States Court of Appeals, Third CircuitScribd Government DocsNo ratings yet
- Final Draft Research PaperDocument6 pagesFinal Draft Research Paperapi-549464161No ratings yet
- 7 Bond and Development Length-SlightDocument47 pages7 Bond and Development Length-Slightريام الموسويNo ratings yet
- Locomotor Movements: NAME: Dannie Anne T. Paynago Year & Section: Bsm-1A Subject: Physical EducationDocument3 pagesLocomotor Movements: NAME: Dannie Anne T. Paynago Year & Section: Bsm-1A Subject: Physical EducationDannie Anne PaynagoNo ratings yet
- Anatomy and Pathophysiology of AnemiaDocument9 pagesAnatomy and Pathophysiology of AnemiaDarlen Rabano88% (8)
- Rede Can Actros 2546 LsDocument8 pagesRede Can Actros 2546 LsAnonymous xxodw3HGP3No ratings yet
- Dryden Natural Springs Case AnalysisDocument3 pagesDryden Natural Springs Case Analysishanna100% (2)
- Ev Exam 3Document9 pagesEv Exam 3Rachelle Danya Dela RosaNo ratings yet
- Security in Project FinanceDocument25 pagesSecurity in Project FinanceIshaya AmazaNo ratings yet
- DOSTOJEVSKI DvojnikDocument13 pagesDOSTOJEVSKI DvojnikVesna RadovanovicNo ratings yet
- Extra homework-Che-XDocument3 pagesExtra homework-Che-XBornil Bikash BhuyanNo ratings yet