408
aaa
Physiology of Labor
PHASES OF PARTURITION. 408
PHASE 1 OF PARTURITION: UTERINE
(QUIESCENCE AND CERVICAL SOFTENING 408
PHASE 2 OF PARTURITION: PREPARATION FOR LABOR. 410,
PHASE 3 OF PARTURITION: LABOR am
PHASE 4 OF PARTURITION: THE PUERPERIUM ay
PHYSIOLOGICAL AND BIOCHEMICAL PROCESSES
REGULATING PARTURITION a7
PHASE 1: UTERINE QUIESCENCE
AND CERVICAL COMPETENCE a9
PHASE 2: UTERINE ACTIVATION AND
CERVICAL RIPENING ‘23
PHASE 3: UTERINE STIMULATION 426
“The last few hours of human pregnancy are characterized by
forceful and painful uterine contractions that effect cervical dle
atation and cause the fetus to descend through the birth canal
“There ate extensive preparations in both the uterus and cervix
long before this. During the fist 36 0 38 weeks of normal gesta-
tion, the myometsium isin a preparatory yet unresponsive state
Concurrency, the cervix begins an early sage of remodeling —
termed sofening—yet maintains structural integrity. Following,
this prolonged uterine quiescence, there is a transitional phase
during which myometrial unresponsiveness is suspended, and
the cervix undergoes ripening, effacement, and los of structural
integrity.
“The physiologieal processes that regulate parturition and the
onset of labor continue to be defined. It is cleat, however, that
labor onset represents the culmination of series of biochemical
changes in the uterus and cervix, These result from endocrine
and paracrine signals emanating from both mother and fetus.
“Their relative contributions vary berween species, nd it ie shese
differences that complicate elucidation of the exact factors
that regulate human parturition. When parturition ie abnor-
‘mal, chen preterm labor, dystocia, of postterm pregnancy may
result, OF these, preterm labor remains the major contributor
to neonatal morcliy and morbidity in developed countries.
PHASES OF PARTURITION
“The bringing forth of young—parturition—requires well-
‘orchestrated transformations in both uterine and cervical fune-
tion. As shown in Figure 21-1, parcurtion can be arbitrarily
divided into four overlapping phases that correspond to the
:ajor physiological wansitions of the myometsium and cervix
luring pregnancy (Casey, 1993, 1997; Challis, 2000; Word,
2007). These phases of parturition include: (1) a prelude to i,
(2) the preparation fo it (3) she process itself, and (4) recovery
Importantly, the phair of parturition should not be confused
with the clinical sages of labor, that is, the fist, second, and
third stages—which comprise the third phase of parturition
(ig. 21-2)
Phase 1 of Parturition: Uterine Quiescence
and Cervical Softening
Uterine Quiescence
Beginning even before implantation, a remarkably effective
petiod of myometrial quiescence is imposed. This phase nor-
rally comprises 95 percent of pregnancy and is characte
ied by werine smooth muscle tanguility with maintenance
‘of cervical structural integrity. The inherent propensity of
the myometrium to conteact is eld in abeyance, and ater
ine muscle is rendered unresponsive to natural stimuli
Concurrently, the uterus must initiate extensive changes in
ite size and vascularity to accommodate the pregnancy and.
Physiology of Labo’
Cervical Softening
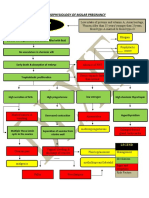
= Fraa Frais —] press] Frame
5 auestsece | _Acivaton_|stmusion | _ alan ‘Tae crv has multiple Functions during
:| Pee Preparation rene Parrot ‘pregnancy that include: (1) maintenance
5 Of barrier Function to pote the repro
5 Contacts} Uterine trie Uterine
rvespasveness | preparedness | contacton, | _ivotute, dlecve tact fom infection, (2) mai
Corea sonenng | “"ertabor | cerca atte, | convalrpa tenance of cevieal competence despite
corvcal | anaptacona| breastfeeding | increasing gravitational forees and’ (3)
cone reorng | expulsn treo crchetraion of extrclllar matic
Initiation of a0 changes that allow progressive increases
Parton Ose in sue compliance
Daler ot ety Tn nonpregnant women, the cervix
(estes is closed and fm, and is consistency
FIGURE 21-1 The phases of patuilion
propare for uterine contractions ‘The myometrial uncespon-
siveness of phase I continues until aca the end of pregnancy.
Some low-intensity myometrial contractions are fle daring
the quiesent phase, but they da not normally cause cervi-
cal dilatation. Contraction of this type become more com
son toward the end of pregnancy, expecially in multiparous
women, and ate referred to as Braxton Hicks contractions or
fale labor (Chap. 4, p. 47)
Stages of Labor
FIGURE 21-2 Composite ofthe average dilatation curve for labor in sully
The curve is based on analysis of data derived ftom 2 large, neatly
women, the fist stage is civided into a relatively lat latent phase
sive active phase Inthe acive phase, there are three identifiable
acceleration phase, a linear ghase af maximum slope, and a dace
from Fiedman, 1978)
is similar to nasal cartilage. By che end
of pregnancy, the cervix is easly disten-
sible, and ite consistency i similar to the lip of the oral cavity
“Thus, che first stage of this remodeling —termed soffening—is
characterized by an increase in tissue compliance, yet the cervix
remains firm and unyielding, Hegar (1895) frst described pal
ppable soltening of the lower uterine segment at 4 co 6 weeks?
sgestation, and this sign was once used co diagnose pregnancy.
Clinically, ehe maintenance of cervical snatomsieal and struc:
cal integrity is essensial for continuation of pregnancy to term.
latation, structural incompetence, of both may
forecast delivery Jams, 1996)
Structural Changes with Softening.
Cervical softening
increased vascularity, stromal. hyper
results from
ant ged
Foal doscont Placonta
twophy, glandular hypertrophy and
‘and deivery. delvery phy, ypertrophy
hyperplasia, and progressive
‘compositional of structural changes of
the extracellular matsix (House, 2009;
Leppert, 1995: Mahendeoo, 2012:
‘Word, 2007). During matrix changes,
collagen, the main structural prosein in
slow,
the cervix, undergoes conformational
changes that alter tissue strength and
flexibility. Specifically. collagen pro-
cessing and the number or type of cova
lent cross-links between collagen tiple
helices are altered, These cross-links
are normally requited for stable col:
lagen fibril formation (Caney, 2005).
A teduetion in. cros
newly synthesized collagen
from reduced expression
and activity of the crose-link forming
‘enzymes, lysyl hydroxylase and lysyl
Jinks berween
oxidase, beginning in eatly pregnancy
(Akins, 2011; Drewes, 2007; Ozasa,
1981). Concurrently there is reduced
expression of the matricelular proceins
thtombospondin 2 and tenascin C.
These proteins also influence collagen
fibril structure and strength. Together,
these early pregnancy changes concrib-
parous women,
consecutive series of
and a rapidly progres
mponent paris: an
ration phase. (
‘ute to the gradual increase in tissue
‘compliance during pregnancy.
409
each Tb)
410
PAN TBES
Labor
“The clinical importance ofthese macrix changes is supported
by the greater prevalence of cervical insufficiency in those with
inherited defects in collagen and elastin synthesis or assem=
bly (Anum, 2009; Hermanns-Lé, 2005: Paternoster, 1998
Rahman, 2003; Wang. 2006). Examples are Ehlers-Danl
and Marfan syndromes, discussed in Chapter 59 (p. 1181).
Additionally, human cervical stromal cells express a transcrip.
tion factor, microphthalmia-astocited transcription factor
(MITF-Cx). During pregnancy, this factor maintains cervical
competency by repressing the expression of genes involved in
cervical dilation and pareurtion (Hari Kishore, 2012).
Phase 2 of Parturition:
Preparation for Labor
‘To prepare for labor, the myometrial tranquility of phase 1
of parturition must be suspended—so-called uterine awakening
ot activation. This phase 2 is a progression of uterine changes
dduting the last 6 to 8 weeks of pregnancy. Importantly, shift
ing events associated with phase 2 can cause either preterm of
delayed labor
Myometrial Changes
Phase 2 myometrial changes prepare it for labor contractions.
‘This shift probably results from alterations in the expression
of key proteins that control conteactiliy, These contraction
‘asociated proteins (CAP) include the oxytocin receptor, pros
taglandin F receptor, and connexin 43 (Smith, 2007). Thus,
myometrial oxytocin receptors markedly increase along with
increased numbers and surface areas of gap junction proteins
such as connexin 43, Together, these lead to increased wer-
ine iriability and responsivences to uterotoninz—agente that
stimulate contractions
‘Another critical change in phase 2 is formation of the lower
uterine segment from the isthmus. With this development,
the fetal head often descend to ot even chtough the pelvic
inlet so-called lightening. The abdomen commonly undergoes
4 shape change, sometimes deseribed by women as “the baby
dropped.” Ics also likely tha che lower segment myomecriurs
is unique from that in the upper uterine segment, resulting
ring labor. This is supported by
differential expression of pros-
receptors within myomettial regions. There are also
‘human studies that report an expression gradient of oxytocin
receptors, with greater expression in fundal myometsial cells
(Fuchs, 1984; Havelock, 2005: Smith, 200
Cervical
Before contractions begin, the cervix must undergo more exten
sive remodeling. ‘This eventually results in cervical yielding
and dilatation upon initiation of forceful uterine contractions
Cervical modifications daring thie second phase principally
involve connective tissue changes—to-called cereal ripening.
“The transition ftom the softening to the ripening phase begins
weeks or days before onset of contractions. During this tans-
formation, the total amount and composition of proteoglycans
and glycosaminoglycans within the matrix are altered. Many
of the processes that aid cervical remodeling are controlled by
the same hormones regulating uterine function. ‘That said, che
molecular events of each are varied because of differences in cel-
lular composition and physiological requirements, The uterine
corpus is predominantly smooth muscle, whereas the cervix is
primarily connective tissue, Cellular components of the cervix
include fibroblasts, epithelia, and few smooth muscle cells.
Endocervical Epithelia
Dring pregnancy, endocervical epithelial cell proliferate
such that endocerveal glands occupy a signitieane pereencage
of cervical mast. The endocervical canal i lined with mucus-
secreting cohumnar and arated squamous epithelia, which
protect against microbial invasion. Mucosal epithelia function
a sentinel fr antigens by expressing Toll-like receptors that
recognize pathogens. In addition, epithelia respond in ways
that lead to bacttial and viral king, For ths, the epithelia
apres antimicrobial peptides and protease inhibitors and sg
nal co underlying immune cells when a pathogenic challenge
cenceede thee protective capacity (Wira, 2005).
Tn mice, studies suggest that cervical epithelia may also aid
cervical remodeling by regulating tissue hydration and main-
tenance of barrier function. Hydration may be regulated by
capresion of aquaporin-—watet channel proteins. Maintenance
of barrie function and paracellular transport of fon and solutes
is regulated by tight junction proteins, such a audins 1 and 2
(Anderson, 2006; Timmons, 2007). Inthe human cevieal and
‘vaginal mucosal epithelia, juneional proteins ae also reported
co be expressed (Blatkewics, 2011)
Cervical Connective Tissue
Collagen. ‘The cervix is an extracellular matrixrich tissue
Constituents of the matrix include type I, I, and IV colla-
gen, elycosaminoglycans, mattieellula proteins, proteoglycans,
and elastin. OF these, collagen is largely responsible for struc
tural disposition of the cervix, Collagen is the most abundant
mammalian protein and has a complex biosynthesis pathway
that includes at lease six enzymes and chaperones to accom
plish macuration. Each collagen
alpha chains, which wind around each other to form procolla-
40. Multiple collagen triple-helial molecules are eross-linked
to one another by the actions of lysyl oxidase to form Abril
Collagen ibis interact with small proscoglyeans such as deco-
rin or biglycan, as well as maticllular proteins such as throm
bospondin 2, These interactions determine fibril size, packing,
and organization (Pig, 21-3). This ensues that collagen fibsis
ate of uniform diameter and are packed together in a regular
and highly organized pattern (Canty, 2005)
Dring cervical ripening, collagen bri diameter is increased,
and there is increased spacing between fibrils. ‘These changes
‘may result in part from accumulation of poorly crosslinked
collagen and reduced expression of matrcellular proteins.
Dispersion of collagen fibrils leads to a loss of tissue ince,
rigy and increased issue compliance, Matrix metalloproteases
(MMPS) ate proteases capable of degrading extracellular mattix
proteins, OF these, collagenase members of the MMP farily
degrade collagen. Some studies support a role of MMPs in
cervical ripening. But, others suggest that the biomechanical
changes are not consistent solely with collagenase aexvation and
cle ie composed of three
Collagen for
/ é \
Fibrl Before During
cervical cervical
feonagen ripening ripening
708s tins
*
Collagen fiber
Tightly packed Cyaan tee
‘ib
Colagen fibar
FIGURE 21-3 Fibila: collagen synthesis and organization. Collagen fis
by small pro!
pening, bail size is uniform, and fibrils are
nized. During cervical ipening, fib size isles uniform, and spacing
into collagen fibers. Fibil size and packing are regulated in p
as decorin that bind collagen. Belote ce
Il packed and o
feen collagen ibis and fib
is increased and disaiganized
loss of collagen. For example, Buhmschi and colleagues (2004)
performed tissue biomechanical studies in the rat and suggest
that ripening coreelases with changes in the three-dimensional
seructure of collagen rather than its degradation by collagenaee.
Moreover, mouse and human studies document no changes in,
collagen content between nonpregnancy and term pregnancy
(Akins, 2011; Myers, 2008: Read, 2007).
‘Thus, ic is likely chat dynamic changes in collagen steue
cure rather than collagen content may regulate cemodeling,
‘This point is well illustrated in specialized microscopy images
of mouse and human cervical collagen (Zhang, 2012). In fur-
ther support, polymoxphisms of mutations in genes required
for collagen assembly are ascciated with an increased incidence
of cervical insufficiency (} 1998;
Rahman, 2003; Warren, 2007
sam, 2009; Paternosce,
Glycosaminoglycans (GAGS). ‘These are high-molecular-
‘weight polysaccharides that complex with proteins to form
proteoglycans, One glycosaminoglyean is hyaluronan (FIA), a
carbohydrate polymer whose synthesis is carried out by hyah
tuonan synthase isoenzymes, Expression of these enzymes is
increased in the cervix during ripening (Akgul, 2012; Osmers,
1993; Stach, 2005). "The functions of hyaluronans are depen
dent on size, and the breakdown of large- to small-molectlar-
weight molecules is carried out by a family of hyaluronidase
enzymes. Hyaluronidase genes are expressed in both the mouse
sed hyaluronidase activity is
reported in the mouse cervix at term (Akgul, 2012). Large-
molecular-weight HA predominates in the mouse cervix during.
ripening and has a dynamic role co increase viscoelasticity and
matrix disorganization, Low-moleculat-weight HA has proin
fammacory properties, and studies in mice and women teveal
increased concentrations during labor and in the puerperium
and human cervix, and incr
Physiology of Labo’
(Akgul, 2012; Ruscheinsky, 2008)
The importance of regulated
changes in HA size during cervical
ripening and distation is supported
by a suudy seporting hyaluronidase
administration to the cervix for
ripening in ttm pregnant women
Gpallicci, 2007). Activaion of,
inacelluar signaling cascades and
other biological functions requites
HA-binding proteins such a versican
‘uscheinsky, 2008)
swith cell-associated
Proteoglycans. ‘These _glycopro:
teins are composed of a protein
core and GAG chains. Changes in
the amount of core protein ot in the
umber, length, oF degree of sul-
fation of GAG chains can influence
proteoglycan function, Although not
well-defined, changesin proteoglycan
composition are thought to accom:
pany cervical ripening. Atleast three
small leucine-rich proteoglycans are
expressed in the cervix—decorin, biglyean, and fibromodulia,
(Westergren-Thorsson, 1998). In other connective tissues, deco
rin and other family members interact with collagen and influ
ence the packing and order of collagen fbrils (Ameye, 2002)
Collagen fibrils are rearranged in the skin of decorin-d
mice and result in collagen fibers that are weakened, shortened,
and disorganized (see Fig. 21-3). In addition to the cervix, these
proteoglycans aze expressed in the fetal membranes and wets.
Changes in expression levels may regulate feral membrane cen-
sile scrength and uterine Function (Meiner, 2007; Wa, 2012).
An
Loosely packed fois
ssemblee
glycans such
Inflammatory Changes. The marked changes within the
estracelhlar matrix during cervical ripening in phase 2 are accom-
panied by stromal invasion wich inflammatory cells."Thishasled to
4 model in which cervical ripening is considered an inflammatory
process. As such, cervical chemoattractants attract inflammatory:
cell, which in tutn release proteases that may aid degradation of
collagen and other matsix components In phase 3 of 4 of part
tion, there is increased cervical expression of chemokines and co:
lagenase/ protease activity. Teas assumed that processes regulating
phases 3 and 4 of dilation and postpartum recovery ofthe cervix
‘were similar to those in phase 2 of cervical ripening (Bokstrom,
1997; Osman, 2003; Sennstrém, 2000; Young, 2002). This has
been challenged by observations from both human and animal
studies. Skamoto and associates (2004, 2005) found no correla-
tion between the degree of clinical cervical ripening and the tesue
concentrations of cervical newtrophilchemoateactant interleukin
8 (ILS), Microarray studies compating gene expression pat
a cerm before and afer cervieal ripening report lite increase in
expression of proinflammatory genes. In contrast, thete isa robust,
increase in proinaramatory and immunosuppressive genes in
the cervix alter delivery compared with during cervical ripening
(GBollapragads, 2009; Hassan, 2006, 2009).
a
each Tb)
an
PAN TBES
Labor
In mouse models, monocyte migration, but not activa-
tion, takes place before labor (Timmons, 2006, 2007, 2009).
Mice deficient in the chemokine receptor CCR2, import
in monocyte homing to tissues, have normally timed lab
“This further supports the suggestion that labs
by an inflammatory response (Menzies, 2012). Furthermore,
issue depletion of neutrophils before birth has no effect on,
the timing oF stecess of parturition, Finally, activation of neu:
wophils, proinflammatory MI macrophages, and alternatively
of activated M2 macrophages is increased within 2 houss after
birth. This suggests a role for inflammatory cells in postpartum,
cervical remodeling and repair.
not initiated
Induction and Prevention of Cervical Ripening
“There ate no therapies to prevent premature cervical ripening,
Cenvieal cerdage is sed to cteumvent cervical insucency,
although success appeats limited (Owen, 2012). In contast,
tteatment to promote cervical ripening for labor induction
includes direct application of prostaglandins E, (PGE,) and
F,, (PGF). Prostaglandins likely modify extracellular matix
structure toa ripening. Although the role of prostaglandins in
the normal physiology of cervical ripening remains uncles, thie
property is wsefl clinically to awa labor induction (Chap. 26,
. 526). In some nonhuman species, che cascades of events that
allow cervical ripening ate induced by deceasng serum proges
tctone concentrations. And in humans, administration of pro
sgesterone ancagonists causes cervial ripening, As discussed late,
humans may have developed unique mechaniame to localize
decreases in progesterone action inthe cervc and rayon
Phase 3 of Parturition: Labor
“This phase is synonymous with active labor, which is custom-
arily divided into three stages. Taese compose the commonly
used labor graph shown in Figute 21-2, The clinical sages of
labor may be summatized as follows, The frst stage begins
when spaced uterine contractions of sufficient frequency, inter
sity, and duration are attained to bring about cervieal thin-
ning, or effacement. This labor stage ends when the cervix is
fally dlaced—about 10 em—to allow passage ofthe term-sized
feeus, The frst stage of labor, cherefoe, isthe stage of cervical
effacement and dilatation
“The cond stage begins when cervical dilatation is complete
and ends with delivery, Thas, the second stage of labor is the
stage of fetal expulsion. Las, the thied stage begins immediately
afier delivery of the fetus and ends with the delivery of the
placenta. Thus, the chi stage of labor is the stage of placental
separation and expubion
First Stage of Labor: Clinical onset of Labor
In some women, forceful uteine contractions that effect deliv-
ery begin suddenly. In othets, labor initiation is heralded by
spontaneous tl amount of blood-tinged mucus
fiom the vagina. This exeuson of the mucus plug that had
previously filled the cervical canal duting pregnancy is referred
to at “show” of “bloody show.” There i very lie blood wich
the macous plug, and its passage indicates that labor i already
in progres or likely wil ensue in hours to day.
Uterine Labor Contractions
‘Unique among physiological muscular contractions, those
‘of uterine smooth muscle during labor ate painful. The
‘cause of this is not known definitely, but several possibilities
have been suggested: (1) hypoxia of the contracted myome-
‘trium—such a5 that with angina pectoris: (2) compression
‘of nerve ganglia in the cervix and lower uterus by contracted
interlocking muscle bundles: (3) cervical stretching during
dilatation; and (4) stretching of the peritoneum overlying
the fundus,
Of these, compression of nerve ganglia in the cervix and
lower uterine segment by the contracting myometrium is an
‘specially attractive hypothesis. Paracervical infiltration wish
local anesthetic usually produces appreciable pain relief with
contractions (Chap. 25, p. 509). Uterine contractions are
involuntary and, for the most part, independent of extra
ine control. Neural blockade from epidural analgesia doce not
diminish their frequency oF intensity. In other examples,
mettial contsactions in paraplegic women and in women aft
bilateral Lumbar sympathectomy are normal but painless,
Mechanical stretching of the cervix enhances uterine aetiv-
ity in several species, ineluding humans. This phenomenon,
hhae been referred to at the Ferguow refex (Ferguson, 1941),
‘exact mechanism i not clear, and release of oxytocin has
been suggested but not proven. Manipulation of the cervix and
“stripping” the fetal membranes is associated with an increase
in blood levels of prostaglandin F,, metabolite (PGEM).
‘The interval between contractions diminishes gradually
from approximately 10 minutes at the onset of first-stage labor
to as little as 1 minute of less in the second stage. Periods of
relaxation berween contractions, however, ae essential for fetal,
welfare. Unremitting contractions compromise uteroplacental
‘blood flow sufficiently to cause fetal hypoxemia. In active-
pphase labor, the duration of each contraction ranges from 30
0 90 seconde, averaging about 1 minute. There is apprecia-
Dle vatiability in contraction intensity during normal labor.
Specifically, amnionie fluid pressures generated by contractions
during spontaneous labor average 40 mm Hg, but vary from 20
eo 60 mm Hg (Chap. 24, p. 498)
Distinct Lower and Upper Uterine Segments. During
active labor, the anatomical uterine divisions that wete ini
tiated in phase 2 of parturition become inereasingly evident
(figs. 21-4 and 21-5). By abdominal palpation, even before
membrane rupture, the swo segments can sometimes be dif-
ferentiated. ‘The upper segment is firm during contractions,
‘whereas the lower segment is softer, distended, and more pas-
sive. This mechanism is imperative because if the entte myo:
metsium, including the lower uterine segment and cervix, were
to contract simultaneously and with equal intensity, the nec
cexpubsive force would be markedly decreased, Thus. the upper
segment contracts, retracts, and expels the fers, In response
tw these contractions, the softened lower uterine segment and
cervix dilate and thereby form a greatly expanded, thinned-out
tube through which the fecus can pass.
The myometrium of the upper segment docs not relax to its
original length after contractions. Instead, it becomes relatively
fixed at a shorter length. ‘The upper active uterine segment
Physiology of Labor
Pathological
retraction
ring (as)
segment
Body.
Physiologica, Paleve
themus. Anat o- ‘retraction ring” segment
Con =, Oblterated 1.0
£o EO. EO:
NONPREGNANT PREGNANT UTERUS INLABOR UTERUS INLABOR UTERUS IN LABOR,
UTERUS UTERUS ATTERM NORMAL. NORMAL “ABNORMAL
EARLY FIRST STAGE, SECOND STAGE SECOND STAGE - DYSTOCIA
FIGURE 21-4 Sequence of development of the segments and rings inthe uterus at term and in labor. Nate comparison between the
uterus of a nonpregnant woman, the uterus at term, and the uterus during labor. the passive lower uterine segment is derived ftom the
isthmus, ané the physiological retraction ring develops atthe junction ofthe upper anc lower uterine segments, the pathological etac-
tian ring develops fram the physiclagical ring. nat, 10, = anatomical internal 95, £.. = extemal a5; Hist 10, = histological internal os,
Ph, R= physiological retraction ring.
contracts down on its diminishing contents, but myomettal
Cension remains constant, The not effect i to cake up slack, thus
maintaining the advantage gained in expulsion of the fetus.
Concurrently, the uterine musculature is kept in firm contact
with the uterine contents. As the consequence of retraction,
cach successive contraction commences where its predecessor
left off ‘Thus, the upper part of the uterine cavity becomes
slightly smaller with each successive contraction. Because of the
suecesive shortening of the muscular fibers, the upper active
segment becomes progressively thickened throughout frst- and
second-stage labor (see Fig. 21-4). This process continues and
results in a tremendously thickened upper uterine segment
immediatly after delivery
Clinically, ic is importane to understand that the phenom-
enon of upper segment retraction is contingent on a decrease in
Passive sogment
“Level of internal cervical os
Cena
— Levelt external earvieal os
Vagina
FIGURE 21-5 The uterus atthe time of vaginal delivery. The
active upper segment retracts around the presenting part as
the fetus descends through the bith canal. Inthe passive lower
segment, there is considerably less myometial one
the volume ofits contents. For this t happen, particularly eatly
in labor when the entire uterus is virtually & closed sac with
only minimal cervical dilatation, che musculacue of che lower
segment must strech. This permits an increasing portion af che
uterine contents co occupy the lower segment. The upper seg-
ment retracts only to the extent that che lower segment distends
and the cervix dilate.
Relaxation of the lower uterine segment mirrors the same
gradual progression of reuaction. Recall chat after each con-
traction of the upper segmens, the muscles do nos return to
thet previous length, but tension remains essentially the same.
By comparison, in the lower segment, successive lengthening.
of the fibers with labor i accompanied by thinning, normally
to only a few millimeters in che chinnest part. As a resule of
the lower segment thinning and concomitant upper segment
thickening, a boundary between the «wo is marked by a ridge
fon the inner uterine surfuce—the phyiolaical retraction ring
‘When the thinning of the lower uterine segment is extreme, as
in obstructed labor, the sing is prominent and forms a patho-
logical reraction ring. This abnortal condition is also known
as the Band! ring, which is discussed further and illustrated in
‘Chapter 23 (p. 470)
‘changes in Uterine Shape During Labor. Each contrac-
tion produces an elongation ofthe ovoid uterine shape with a
concomitant dectease in horizontal diameter. This change in
shape has importanc effects on the labor process. Fist, there
is increased fetal axis presur, that is, the decreased horizontal
diameter serves to sisighten the fea vertebral column. This
prestes the upper pole of che ferus firmly against the fundus,
‘whereas the lower pole is thrust farther downward. The lengsh-
‘ening of the ovoid shape has been estimated at 5 and 10 em.
Second, with lengthening ofthe uterus, the longitudinal muscle
fibers are drawn taut. As a result, the lower segment and cervix
are the only parts of the uterus that are flexible, and these are
polled upward and around the lower pole ofthe fetus
Ancillary Forces in Labor
‘Ace the cervix is dilated fully, the most imporcant foree in
fetal expulsion is that produced by maternal intrsabdominal
a3
each Tb)
a4
PAN TBES
Labor
Pressure, Contraction of the abdominal muscles simultane-
‘ously with forced respiratory efforts with the glotis closed is
referred to as pushing. ‘The force is similar wo that with def
cation, but the intensity usually is much greater. The impor-
tance of intsaabdominal pressure is shown by the prolonged
descent during labor in paraplegic women and in those with a
dense epidusal block. And, although increased intraabdominal
pressure is necessary to complete second-stage labor, pushing
accomplishes lite in the frst stage. Itexhauss the mother, and
its associated inereased intrauterine pressures may be harmfil
co the fees.
Cervical Changes
‘As the result of contraction forces, two fundamental changes—
‘effacement and dilatation —oeeur in the alteady-ripened cervix.
For an average-sied fetal head co pass through the cervix, its
‘anal must dilace to a diameter of approximately 10 cm. Ac
this time, the cervix is said to be completely or fly dilated.
Although there may be no fetal descent during cervical efface-
ment, most commonly the presenting fetal part descends
somewhat as the cervix dilates. During second-stage labor in
nullipaas, the presenting part «ypically descends slowly and
steadily. In multiparas, however, particularly those of high parity,
descent may be rapid.
Cervical elacement is “obliteration” ot “taking up” of the
cervix, It is manifest clinically by shortening of the cervical
Muttpara Primigravia
FIGURE 21-6 Schematic showing effacement and dilatation
‘A. Before labo, the primigravid cervix is lang and undated in
«contrast to that of the mutipaa, which has dilatation of the inter=
nal and external os, B. AS effacement begins, the mutiparous
You might also like
- Fever and HyperthermiaDocument6 pagesFever and HyperthermiaMarco Paulo Reyes NaoeNo ratings yet
- Physiology Index CardsDocument30 pagesPhysiology Index CardsMarco Paulo Reyes NaoeNo ratings yet
- Ob-Gyn Post Graduate Interns May-June 2017-2018Document1 pageOb-Gyn Post Graduate Interns May-June 2017-2018Marco Paulo Reyes NaoeNo ratings yet
- Alcoholic Liver DiseaseDocument22 pagesAlcoholic Liver DiseaseVikramjeet SinghNo ratings yet
- SEIZURE CASE PROTOCOLDocument1 pageSEIZURE CASE PROTOCOLMarco Paulo Reyes NaoeNo ratings yet
- Williams Endocrinology Large CoverDocument1 pageWilliams Endocrinology Large CoverMarco Paulo Reyes Naoe33% (9)
- Table of Contents Williams Endocrinology 13th EditionDocument4 pagesTable of Contents Williams Endocrinology 13th EditionMarco Paulo Reyes NaoeNo ratings yet
- Assessment of Back Pain-BMJDocument30 pagesAssessment of Back Pain-BMJMarco Paulo Reyes NaoeNo ratings yet
- Electronic Chapter Harrison's 19th EditionDocument1 pageElectronic Chapter Harrison's 19th EditionMarco Paulo Reyes Naoe0% (1)
- Gradeschool ReviewerDocument7 pagesGradeschool ReviewerMarco Paulo Reyes NaoeNo ratings yet
- APRIL 2017: Aurora Hill and Engineer's Hill Health CentersDocument2 pagesAPRIL 2017: Aurora Hill and Engineer's Hill Health CentersMarco Paulo Reyes NaoeNo ratings yet
- Pharma Super TableDocument56 pagesPharma Super TableMarco Paulo Reyes NaoeNo ratings yet
- Gastroenterology-Liver, Pancreas and Gall Bladder LecturesDocument7 pagesGastroenterology-Liver, Pancreas and Gall Bladder LecturesMarco Paulo Reyes NaoeNo ratings yet
- Approach to Leg Edema DiagnosisDocument4 pagesApproach to Leg Edema DiagnosisMarco Paulo Reyes NaoeNo ratings yet
- CPC NarrationDocument5 pagesCPC NarrationMarco Paulo Reyes NaoeNo ratings yet
- Acute Nephritic SyndromeDocument1 pageAcute Nephritic SyndromeMarco Paulo Reyes NaoeNo ratings yet
- Price List For PVC Single Loop Wire From OREZADocument1 pagePrice List For PVC Single Loop Wire From OREZAMarco Paulo Reyes NaoeNo ratings yet
- Special Awards - ListDocument7 pagesSpecial Awards - ListMarco Paulo Reyes NaoeNo ratings yet
- Cancer Drugs MRSDocument12 pagesCancer Drugs MRSMarco Paulo Reyes NaoeNo ratings yet
- Liver Cirrhosis2 LectureDocument104 pagesLiver Cirrhosis2 LectureMarco Paulo Reyes NaoeNo ratings yet
- Selective Serotonin Reuptake Inhibitors: Naoe, Marco Paulo RDocument38 pagesSelective Serotonin Reuptake Inhibitors: Naoe, Marco Paulo RMarco Paulo Reyes NaoeNo ratings yet
- Florist ContractDocument1 pageFlorist ContractMarco Paulo Reyes NaoeNo ratings yet
- Pharma AntidiarrhealDocument3 pagesPharma AntidiarrhealMarco Paulo Reyes NaoeNo ratings yet
- CPC SCRIPT SemifinalDocument5 pagesCPC SCRIPT SemifinalMarco Paulo Reyes NaoeNo ratings yet
- Admiting Conference - Acute GastroenteritisDocument38 pagesAdmiting Conference - Acute GastroenteritisMarco Paulo Reyes NaoeNo ratings yet
- Consent in Emergency CasesDocument10 pagesConsent in Emergency CasesMarco Paulo Reyes NaoeNo ratings yet
- Pharma AntidiarrhealDocument3 pagesPharma AntidiarrhealMarco Paulo Reyes NaoeNo ratings yet
- 3rd and 4th Stage of Labor Dr. BaduaDocument8 pages3rd and 4th Stage of Labor Dr. BaduaMarco Paulo Reyes NaoeNo ratings yet
- Adrenal Glands: I. Historical BackgroundDocument7 pagesAdrenal Glands: I. Historical BackgroundMarco Paulo Reyes NaoeNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- s5 Michelle M. Ramos - Science 5 Describe The Part of Human Reproductive System and Their FunctionfinalDocument14 pagess5 Michelle M. Ramos - Science 5 Describe The Part of Human Reproductive System and Their FunctionfinalRandolf Cruz100% (7)
- Human Growth SEM-01 - A1Document85 pagesHuman Growth SEM-01 - A1ggsachary100% (1)
- Care of Mother, Child, and Adolescent: Prepared by Donna Belle Sumugat RN ManDocument26 pagesCare of Mother, Child, and Adolescent: Prepared by Donna Belle Sumugat RN ManLaurence Docog100% (1)
- Partial Mole or Complete Mole: Pathophysiology of Molar PregnancyDocument1 pagePartial Mole or Complete Mole: Pathophysiology of Molar PregnancyKristian Karl Bautista Kiw-isNo ratings yet
- Optimizing Breastfeeding For Better Health Outcomes The Way ForwardDocument4 pagesOptimizing Breastfeeding For Better Health Outcomes The Way ForwardEditor IJTSRDNo ratings yet
- Maternal Placental Foetal UnitDocument10 pagesMaternal Placental Foetal UnitFestus SinoNo ratings yet
- Informed Consent For Anesthesia CareDocument22 pagesInformed Consent For Anesthesia CareCatherine MorrisNo ratings yet
- Oral Contraceptive MCQs With Answer KeyDocument7 pagesOral Contraceptive MCQs With Answer KeyShaista AkbarNo ratings yet
- Sci PPT Q2 WK 2 Day 1-5Document74 pagesSci PPT Q2 WK 2 Day 1-5mary antonette pagalNo ratings yet
- Endometritis PDFDocument3 pagesEndometritis PDFNur azizah FitriyanaNo ratings yet
- Jaundice in Pregnancy: M2 - Fmbs DR Dohbit Sama Prof Mboudou E. TDocument35 pagesJaundice in Pregnancy: M2 - Fmbs DR Dohbit Sama Prof Mboudou E. TSerge TresorNo ratings yet
- Journal Critiquing Article Reviewed:: Submitted To: Prof. Cynthia A. Umila, RN, MAN Submitted By: Yvette Claire L. BorresDocument6 pagesJournal Critiquing Article Reviewed:: Submitted To: Prof. Cynthia A. Umila, RN, MAN Submitted By: Yvette Claire L. BorresYVETTE CLAIRE BORRESNo ratings yet
- Medical TerminationDocument6 pagesMedical TerminationRadha SriNo ratings yet
- Maternal Child Nursing Care in Canada 2Nd Edition Perry Test Bank Full Chapter PDFDocument36 pagesMaternal Child Nursing Care in Canada 2Nd Edition Perry Test Bank Full Chapter PDFChristopherHugheswpya100% (10)
- Data AnalysisDocument1 pageData AnalysisRicardoNo ratings yet
- Management of Normal Labor and Delivery - UpToDateDocument46 pagesManagement of Normal Labor and Delivery - UpToDateTrần Ngọc BíchNo ratings yet
- Endocrine SystemDocument28 pagesEndocrine Systemdrin zekaNo ratings yet
- Fundamentals of ReproductionDocument4 pagesFundamentals of ReproductionHalo Ini JeskryNo ratings yet
- Apgar and BallardDocument16 pagesApgar and Ballardcarlos ponceNo ratings yet
- Delivery PackageDocument2 pagesDelivery Packageemailriturajsaxena1No ratings yet
- B11 Hormonal Coordination Exam-Style QuestionsDocument7 pagesB11 Hormonal Coordination Exam-Style QuestionsDevangi VyasNo ratings yet
- Pathophysiology of Varicose VeinsDocument2 pagesPathophysiology of Varicose VeinsKim SunooNo ratings yet
- Literature Review JaundiceDocument7 pagesLiterature Review Jaundicec5t0jsyn100% (1)
- A Roman Catholic View of Population ControlDocument25 pagesA Roman Catholic View of Population ControlAron MarielNo ratings yet
- High Risk PregnancyDocument113 pagesHigh Risk PregnancyVivian Lajara100% (2)
- Philippine Traditions and PracticesDocument15 pagesPhilippine Traditions and PracticesJohn Carlo Dela CruzNo ratings yet
- Theories, Models and Approaches Applied To Midwifery PracticesDocument111 pagesTheories, Models and Approaches Applied To Midwifery Practicesdr.anu Rk90% (10)
- Medication for Rhogam and ITPDocument1 pageMedication for Rhogam and ITPAA DDNo ratings yet
- Poor Hygiene and Health Risks in a FamilyDocument10 pagesPoor Hygiene and Health Risks in a FamilyJeffer Dancel67% (3)
- Chapter 018Document12 pagesChapter 018api-281340024No ratings yet