You might also like
- Opioid Mortality: and Selected TrendsDocument7 pagesOpioid Mortality: and Selected TrendsWIS Digital News StaffNo ratings yet
- Ticket To Ride Route Point EfficiencyDocument1 pageTicket To Ride Route Point EfficiencyhenriquevccangussuNo ratings yet
- Ohio State Highway Patrol Citations For Securing Loads On VehiclesDocument1 pageOhio State Highway Patrol Citations For Securing Loads On VehiclesAnonymous DiwQWkbHNo ratings yet
- TSP (C)Document1 pageTSP (C)Vakul KhullarNo ratings yet
- Cluster For ClassDocument1 pageCluster For ClassJuhi BhattacharjeeNo ratings yet
- MLB AttendanceDocument1 pageMLB AttendanceJohn HallNo ratings yet
- MLB AttendanceDocument1 pageMLB AttendanceJohn HallNo ratings yet
- Opioid Deaths All TownsDocument10 pagesOpioid Deaths All TownsHelen BennettNo ratings yet
- DK-Lok Tubing Fittings DMC-NDocument1 pageDK-Lok Tubing Fittings DMC-Ngohjh80No ratings yet
- US City Demographic Cluster AnalysisDocument8 pagesUS City Demographic Cluster AnalysisSwetha ThotaNo ratings yet
- %age Black %age Hispanic %age Asian Median Age Unemployment Rate Per Capita Income (000's)Document8 pages%age Black %age Hispanic %age Asian Median Age Unemployment Rate Per Capita Income (000's)NipunNo ratings yet
- 1882-1889 Whitman WA Precinct Level Election ResultsDocument66 pages1882-1889 Whitman WA Precinct Level Election ResultsJohn MNo ratings yet
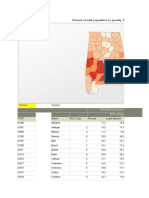
- Percent Number: All People in Poverty (2016) 90% Confidence Interval of EstimateDocument6 pagesPercent Number: All People in Poverty (2016) 90% Confidence Interval of EstimateAshok GuntupalliNo ratings yet
- SW0010Document2 pagesSW0010BittuNo ratings yet
- Massachusetts Opioid Deaths by County Nov-17Document2 pagesMassachusetts Opioid Deaths by County Nov-17Ashley ShookNo ratings yet
- Plano TelecasterDocument1 pagePlano TelecasterMago El CrakNo ratings yet
- County Sheriff CCW ReportDocument1 pageCounty Sheriff CCW ReportDean0No ratings yet
- IndextempDocument1 pageIndextempauhonaNo ratings yet
- BP Total Monthly Family Units by Sector, FY13-FY17Document5 pagesBP Total Monthly Family Units by Sector, FY13-FY17Paul M. IngramNo ratings yet
- Table 10 Offenses Known To Law Enforcement Arkansas by Metropolitan and Nonmetropolitan Counties 2017Document3 pagesTable 10 Offenses Known To Law Enforcement Arkansas by Metropolitan and Nonmetropolitan Counties 2017매직키보드No ratings yet
- 1992-93 Phoenix Suns Media Guide Phoenix Suns P - B071CQBX7V PDFDocument212 pages1992-93 Phoenix Suns Media Guide Phoenix Suns P - B071CQBX7V PDFlevine2001No ratings yet
- Q3Document1 pageQ3RamanNo ratings yet
- SK Ajar Cluster 2021Document2 pagesSK Ajar Cluster 2021AFDHAL PASANo ratings yet
- SSMD - Session 5 - ExcelDocument11 pagesSSMD - Session 5 - ExcelHarish GangardeNo ratings yet
- ASCE 7-22 CH 07com - For PC - SouDocument66 pagesASCE 7-22 CH 07com - For PC - SousharethefilesNo ratings yet
- David Rillie Paternity TestDocument1 pageDavid Rillie Paternity TestJulie WolfeNo ratings yet
- Elon Musk Deposition - SolarCity and Tesla Model 3Document78 pagesElon Musk Deposition - SolarCity and Tesla Model 3Bryan Logan100% (1)
- State Number of Public Grants Number of Public LibrariesDocument4 pagesState Number of Public Grants Number of Public Librariessandeeppradeep123No ratings yet
- Session 28 - Timeseries AnalysisDocument13 pagesSession 28 - Timeseries AnalysisDHARSHNI P GRGSMSNo ratings yet
- DNA Test Report TitleDocument1 pageDNA Test Report TitleAnuj AlexNo ratings yet
- IndextempDocument2 pagesIndextempauhonaNo ratings yet
- Land Survey Plat Index - 202205191514250336Document52 pagesLand Survey Plat Index - 202205191514250336GmVNo ratings yet
- Lucarea 2 Metoda in ParalelDocument24 pagesLucarea 2 Metoda in ParalelDaniel Ionut BudaesNo ratings yet
- Simpson, ChristopherDocument1 pageSimpson, ChristophermypenguyNo ratings yet
- 2017 125 Open Champ. Points After DonigtonDocument1 page2017 125 Open Champ. Points After DonigtonPhil FeatherstoneNo ratings yet
- R3G CalendarDocument26 pagesR3G CalendarHirmann YubNo ratings yet
- STC 1.2 Points GPM ResultsDocument1 pageSTC 1.2 Points GPM ResultsKopacz GyulaNo ratings yet
- Derek HorshamDocument2 pagesDerek HorshamrnvrNo ratings yet
- Report To The Colorado General Assembly 2008Document2 pagesReport To The Colorado General Assembly 2008Dean0No ratings yet
- Rata Incidenta Covid 19 17 10 2021Document2 pagesRata Incidenta Covid 19 17 10 2021jeanina lupuNo ratings yet
- Distance Between Chicago and Miami Disnace Between Seattle and Dallas Suppose You Visit Cities in Following Order, City 8-7-5-4-3-2-8Document2 pagesDistance Between Chicago and Miami Disnace Between Seattle and Dallas Suppose You Visit Cities in Following Order, City 8-7-5-4-3-2-8sivaji_ssNo ratings yet
- Triple CrownDocument2 pagesTriple CrowndanielmulliganNo ratings yet
- Air PollDocument6 pagesAir PollSantiago MolanoNo ratings yet
- Mda-Session-7 Simple Linear RegressionDocument75 pagesMda-Session-7 Simple Linear RegressionArijit Dutta 210075698No ratings yet
- HSFB Vine MVL 1126Document2 pagesHSFB Vine MVL 1126Ben WatanabeNo ratings yet
- Ms ExcelDocument106 pagesMs Excellisa leeNo ratings yet
- Empire Service: New York Niagara Falls - and - TorontoDocument4 pagesEmpire Service: New York Niagara Falls - and - Torontobilbobaggins272722No ratings yet
- Bay Area Council PollDocument9 pagesBay Area Council PollBayAreaNewsGroupNo ratings yet
- The 2017 Bay Area Council Poll Web Survey of 9-County Bay Area Registered Voters EMC Research #17-6284 Conducted January 24 - February 1, 2017 N 1000Document9 pagesThe 2017 Bay Area Council Poll Web Survey of 9-County Bay Area Registered Voters EMC Research #17-6284 Conducted January 24 - February 1, 2017 N 1000Zerohedge0% (1)
- Ms ExcelDocument106 pagesMs Excellisa leeNo ratings yet
- February 2, 2009Document20 pagesFebruary 2, 2009api-19794849No ratings yet
- Ste 2.2 Points GPM ResultsDocument1 pageSte 2.2 Points GPM ResultsAttila DarvasNo ratings yet
- Ste 1.2 Points GPM ResultsDocument1 pageSte 1.2 Points GPM ResultsKopacz GyulaNo ratings yet
- Grading Sheet 2018-2019 AGUINALDODocument104 pagesGrading Sheet 2018-2019 AGUINALDONylremle AsesorNo ratings yet
- City distance matrix analysisDocument6 pagesCity distance matrix analysisLourdes CagungunNo ratings yet
- Monthly expenses and payments scheduleDocument3 pagesMonthly expenses and payments schedulesubaash libraNo ratings yet
- Best Places For Business and Careers: Special ReportDocument8 pagesBest Places For Business and Careers: Special Reportrichc.usNo ratings yet
- Spread SheetDocument1 pageSpread SheetMichael BatesNo ratings yet
- Municipality Notes RRE Comm PP MV: FY 2019 Rhode Island Tax Rates by Class of PropertyDocument1 pageMunicipality Notes RRE Comm PP MV: FY 2019 Rhode Island Tax Rates by Class of PropertyAnonymous twcKq4No ratings yet
- Empirical Dynamic Asset Pricing: Model Specification and Econometric AssessmentFrom EverandEmpirical Dynamic Asset Pricing: Model Specification and Econometric AssessmentRating: 4.5 out of 5 stars4.5/5 (3)
- Omb Bulletin No. 06-01Document2 pagesOmb Bulletin No. 06-01losangeles100% (1)
- 02370-b06-01 Rev 2Document152 pages02370-b06-01 Rev 2losangelesNo ratings yet
- Executive Office of The President Office ofDocument9 pagesExecutive Office of The President Office oflosangeles100% (1)
- Executive Office of The President: Attachment BDocument5 pagesExecutive Office of The President: Attachment Blosangeles100% (1)
- 02368-b06-01 CorrectionDocument1 page02368-b06-01 Correctionlosangeles100% (1)
- Executive Office of The President Executive Office of The PresidentDocument4 pagesExecutive Office of The President Executive Office of The Presidentlosangeles100% (1)
- 02359-b04-03 AppendixDocument146 pages02359-b04-03 AppendixlosangelesNo ratings yet
- 02366-b05-02 AttachmentDocument2 pages02366-b05-02 Attachmentlosangeles100% (1)
- 02360-b04-03 AttachmentDocument5 pages02360-b04-03 AttachmentlosangelesNo ratings yet
- 02359-b04-03 AppendixDocument146 pages02359-b04-03 AppendixlosangelesNo ratings yet
- Executive Office of The President Executive Office of The PresidentDocument13 pagesExecutive Office of The President Executive Office of The Presidentlosangeles100% (1)
- 02358-b04-02 Supp1Document7 pages02358-b04-02 Supp1losangelesNo ratings yet
- b04 04Document16 pagesb04 04losangeles100% (1)
- 02361-b04-03 ErrataDocument1 page02361-b04-03 Erratalosangeles100% (1)
- Executive Office of The PresidentDocument23 pagesExecutive Office of The Presidentlosangeles100% (1)
- b04 02Document12 pagesb04 02losangelesNo ratings yet
- b02 06add1Document7 pagesb02 06add1losangelesNo ratings yet
- Executive Office of The President: What Are The Legal Authorities Under Which OMB Is Requiring Agency Action?Document3 pagesExecutive Office of The President: What Are The Legal Authorities Under Which OMB Is Requiring Agency Action?losangelesNo ratings yet
- b03 01Document23 pagesb03 01losangelesNo ratings yet
- b03 02Document7 pagesb03 02losangelesNo ratings yet
- b02 02Document13 pagesb02 02losangelesNo ratings yet
- Attachment BDocument4 pagesAttachment BlosangelesNo ratings yet
- Executive Office of The President Executive Office of The PresidentDocument5 pagesExecutive Office of The President Executive Office of The PresidentlosangelesNo ratings yet
- Executive Office of The PresidentDocument20 pagesExecutive Office of The PresidentlosangelesNo ratings yet
- 02352-b03-04 AttachDocument141 pages02352-b03-04 AttachlosangelesNo ratings yet
- b02 06a2Document8 pagesb02 06a2losangelesNo ratings yet
- b01 04Document6 pagesb01 04losangelesNo ratings yet
- b02 05Document8 pagesb02 05losangelesNo ratings yet
- b02 06Document8 pagesb02 06losangelesNo ratings yet
- b01 05Document2 pagesb01 05losangelesNo ratings yet
- A prayer for comfort in griefDocument3 pagesA prayer for comfort in griefDReyesNo ratings yet
- Idi Debrief Pre-Test ResultsDocument11 pagesIdi Debrief Pre-Test Resultsapi-263459278No ratings yet
- Pegging and The Heterosexualization of Anal Sex: An Analysis of SavageDocument18 pagesPegging and The Heterosexualization of Anal Sex: An Analysis of SavagepurepresenceNo ratings yet
- Principles of Management 1: Chapter One Part 3: Management HistoryDocument17 pagesPrinciples of Management 1: Chapter One Part 3: Management HistoryWalaa ElsharifNo ratings yet
- Disha Quick Revision English Core MindMaps C 12 @crackjee XyzDocument32 pagesDisha Quick Revision English Core MindMaps C 12 @crackjee XyzSubhrajyoti BanerjeeNo ratings yet
- Positive Attitude in Tourism Industry - 2015Document48 pagesPositive Attitude in Tourism Industry - 2015Meryjoy MesaNo ratings yet
- Child Health Problems, Under 5 Clinic, Delivery of MCH ServicesDocument23 pagesChild Health Problems, Under 5 Clinic, Delivery of MCH ServicesNidhi KaushalNo ratings yet
- 7512993Document4 pages7512993ShubhamNo ratings yet
- Tipología en ArquitecturaDocument276 pagesTipología en ArquitecturaVladislav01No ratings yet
- Dialogue Script Between The A Bcba and ClientDocument3 pagesDialogue Script Between The A Bcba and Clientcrystal mcintoshNo ratings yet
- Antoinette Fox 1Document63 pagesAntoinette Fox 1CAILNo ratings yet
- Time Zones Placement Test: To The TeacherDocument1 pageTime Zones Placement Test: To The TeacherDanilo OliveiraNo ratings yet
- Testing Reading Comprehension in Medical English TeachingDocument12 pagesTesting Reading Comprehension in Medical English TeachingAraceli RiveraNo ratings yet
- Reflective Practice: The Foundation of Purposeful LearningDocument14 pagesReflective Practice: The Foundation of Purposeful LearningHatem FaroukNo ratings yet
- Sections, Parts and ChaptersDocument3 pagesSections, Parts and ChaptersRonald De CastroNo ratings yet
- Presented By: Anuja Saxena Disha Satsangi Lovely Tripti SinghDocument19 pagesPresented By: Anuja Saxena Disha Satsangi Lovely Tripti SinghTripti SinghNo ratings yet
- EthicsDocument6 pagesEthicsCess UrrizaNo ratings yet
- LP About Multimodal and Its ElementsDocument7 pagesLP About Multimodal and Its ElementsAdelaide RefugioNo ratings yet
- Project LeadershipDocument50 pagesProject LeadershipShalini Agarwal100% (1)
- The Intersection of History, Literature and Trauma in Chimamanda Ngozi Adichie's HalfDocument60 pagesThe Intersection of History, Literature and Trauma in Chimamanda Ngozi Adichie's HalfHouda BoursNo ratings yet
- Types of Training and Its BenefitsDocument12 pagesTypes of Training and Its BenefitsNajmiNo ratings yet
- Bmem-Ethics For Managers Final Exam-December 2018Document3 pagesBmem-Ethics For Managers Final Exam-December 2018Jenipher KalembelaNo ratings yet
- BorderlineDocument368 pagesBorderlinenatureinnovator100% (15)
- Diaspora Action Australia Annual Report 2012-13Document24 pagesDiaspora Action Australia Annual Report 2012-13SaheemNo ratings yet
- Sample Af Form 860aDocument2 pagesSample Af Form 860aelsalenNo ratings yet
- Final Essay - Signature AssignmentDocument6 pagesFinal Essay - Signature Assignmentapi-600669880No ratings yet
- Module 8Document5 pagesModule 8api-507793249No ratings yet
- Creative Economy PDFDocument39 pagesCreative Economy PDFMarco MallamaciNo ratings yet
- UnityDocument39 pagesUnitymonalNo ratings yet
- Utah Studies Disclosure 2017Document3 pagesUtah Studies Disclosure 2017api-292396788No ratings yet