You might also like
- Peds OspeDocument85 pagesPeds OspeMin Maw60% (5)
- Ospe 2Document31 pagesOspe 2Med StudentNo ratings yet
- Pediatric OSCE MBBS Final Year Examination: College of Medical Sciences Teaching Hospital Bharatpur, Chitwan 2018Document6 pagesPediatric OSCE MBBS Final Year Examination: College of Medical Sciences Teaching Hospital Bharatpur, Chitwan 2018Ram Pokharel100% (1)
- Pediatric OSCE Pictures: For UndergraduatesDocument70 pagesPediatric OSCE Pictures: For UndergraduatesShehab MhmdNo ratings yet
- Osce PG 1Document18 pagesOsce PG 1Mobin Ur Rehman Khan100% (1)
- Guide to Pediatric Clinical Examination and AssessmentDocument150 pagesGuide to Pediatric Clinical Examination and AssessmentDr.P.NatarajanNo ratings yet
- King's Paediatric Case Studies GuideDocument28 pagesKing's Paediatric Case Studies GuideboblishNo ratings yet
- Aiims - Pediatrics Q&ADocument207 pagesAiims - Pediatrics Q&AqqypprcyxyNo ratings yet
- Paediatrics Triple A-1 PDFDocument120 pagesPaediatrics Triple A-1 PDFparekhpragnesh100% (1)
- Ospe For Revision ClassDocument128 pagesOspe For Revision ClassHaseeb Sadi100% (3)
- HX Taking of PeadiatricsDocument5 pagesHX Taking of PeadiatricsCahaya Al-Hazeenillah100% (1)
- Pediatrics Oral ExamDocument13 pagesPediatrics Oral ExamOmar Nayef TaaniNo ratings yet
- 09-Pediatrics in Review, September2009 PDFDocument71 pages09-Pediatrics in Review, September2009 PDFMobin Ur Rehman KhanNo ratings yet
- Tmbool's Notes in Obstetrics and Gynecology PDFDocument113 pagesTmbool's Notes in Obstetrics and Gynecology PDFOsman SomiNo ratings yet
- Gynaecology History Taking GuideDocument7 pagesGynaecology History Taking GuideJahangir AlamNo ratings yet
- OSPE EXAM OF OBSTETRICS AND GYNAECOLOGY (AFMG 2017/2018Document43 pagesOSPE EXAM OF OBSTETRICS AND GYNAECOLOGY (AFMG 2017/2018Nabilah Mohammad KhalisNo ratings yet
- All Pediatrics 2Document200 pagesAll Pediatrics 2niemand daNo ratings yet
- Pediatric OSCEDocument153 pagesPediatric OSCEAtria DewiNo ratings yet
- Combined Orals APGODocument52 pagesCombined Orals APGOEmilee Tu0% (1)
- كامل نساءDocument181 pagesكامل نساءYasser ArefNo ratings yet
- Diarrhea (Ped) DDX - Gastroenteritis - Food Poisoning - Uti - Uri - Cow Milk Protein Allergy Dopcsfaaa AbcoDocument34 pagesDiarrhea (Ped) DDX - Gastroenteritis - Food Poisoning - Uti - Uri - Cow Milk Protein Allergy Dopcsfaaa AbcofeawefNo ratings yet
- Paediatric Examination Handbook 2015Document66 pagesPaediatric Examination Handbook 2015Ulfa Rahmadanti SetiawanNo ratings yet
- Toacs 8Document305 pagesToacs 8Mobin Ur Rehman Khan100% (2)
- Toacs 6Document159 pagesToacs 6Mobin Ur Rehman Khan100% (2)
- BMLE SecretsDocument224 pagesBMLE SecretsAli Al.Juffairi75% (4)
- Pediatrics One Liner For TestDocument2 pagesPediatrics One Liner For TestArvindhanNo ratings yet
- Paediatric Rashes: Ali Faisal SaleemDocument51 pagesPaediatric Rashes: Ali Faisal Saleemarjumand100% (2)
- Gyne Case COCDocument37 pagesGyne Case COCLian BaylosisNo ratings yet
- Pediatrics OSCEDocument3 pagesPediatrics OSCEMoh'd Ghanayem100% (1)
- Clinical Guidelines in PediatricsDocument267 pagesClinical Guidelines in PediatricsDrshaukat N PanjawaniNo ratings yet
- Pediatrics History Taking PDFDocument2 pagesPediatrics History Taking PDFamarch517100% (1)
- Essential Revision Notes in Paediatrics For The MRCPCH From PastestDocument7 pagesEssential Revision Notes in Paediatrics For The MRCPCH From Pastestarshad100% (1)
- Basic Sciences For MRCPCH ExamDocument11 pagesBasic Sciences For MRCPCH ExamMahmoud Abul AtaNo ratings yet
- PEDIATRICS NOTES LEGAL ISSUES PHYSICAL EXAMDocument64 pagesPEDIATRICS NOTES LEGAL ISSUES PHYSICAL EXAMrvar839100% (2)
- Pediatrics PG Exam PapersDocument39 pagesPediatrics PG Exam Paperscooldude_secbad1712100% (1)
- اذكرونا بدعوة Pediatric Theory Final ExamDocument23 pagesاذكرونا بدعوة Pediatric Theory Final ExamSarwar Sarkawt100% (1)
- Toacs 2Document215 pagesToacs 2Mobin Ur Rehman Khan100% (1)
- Pediatrics Examination ReviewDocument223 pagesPediatrics Examination Reviewgarlic100100% (15)
- Pediatric History Taking and Physical ExamDocument32 pagesPediatric History Taking and Physical ExamCJ Tee100% (1)
- PRO III 2012 Long Case (Surgical)Document39 pagesPRO III 2012 Long Case (Surgical)vijayaNo ratings yet
- Pediatrics Question PaperDocument21 pagesPediatrics Question Paperprinceej100% (3)
- Pediatric Department Book Part 1 (2019-2020)Document260 pagesPediatric Department Book Part 1 (2019-2020)Mohammed Arar100% (1)
- Pediatrics BookDocument53 pagesPediatrics BookMobin Ur Rehman Khan100% (1)
- OSCE recalls 2011, 2013, 2016 gynaecology and obstetrics topicsDocument6 pagesOSCE recalls 2011, 2013, 2016 gynaecology and obstetrics topicsFA Khan100% (1)
- 2 Year Old / M: What Is Your Diagnosis?Document31 pages2 Year Old / M: What Is Your Diagnosis?Mobin Ur Rehman Khan100% (1)
- Essential Revision Notes in Paediatrics For The MRCPCH Third EditionDocument26 pagesEssential Revision Notes in Paediatrics For The MRCPCH Third EditionNadejda MarcovaNo ratings yet
- Ospe Bank PDFDocument318 pagesOspe Bank PDFMed StudentNo ratings yet
- Clinical Pediatric PDFDocument300 pagesClinical Pediatric PDFfloare de coltNo ratings yet
- Pediatrics Solved WBUHS Question Papers PDFDocument162 pagesPediatrics Solved WBUHS Question Papers PDFγιαννης παπαςNo ratings yet
- Toronto Notes DermatologyDocument52 pagesToronto Notes Dermatologyalphabeta101100% (1)
- Best Patient History (US)Document2 pagesBest Patient History (US)John RusNo ratings yet
- Pediatric 6th Year 2016Document30 pagesPediatric 6th Year 2016motasem alsharifNo ratings yet
- PediatricsDocument80 pagesPediatricsakufahaba100% (2)
- The Unofficial Guide to Obstetrics and Gynaecology: Core O&G Curriculum Covered: 300 Multiple Choice Questions with Detailed Explanations and Key Subject SummariesFrom EverandThe Unofficial Guide to Obstetrics and Gynaecology: Core O&G Curriculum Covered: 300 Multiple Choice Questions with Detailed Explanations and Key Subject SummariesRating: 1.5 out of 5 stars1.5/5 (3)
- Comprehensive Handbook Obstetrics & Gynecology 3rd EdFrom EverandComprehensive Handbook Obstetrics & Gynecology 3rd EdRating: 5 out of 5 stars5/5 (1)
- The Unofficial Guide to Paediatrics: Core Curriculum, OSCEs, clinical examinations, practical skills, 60+ clinical cases, 200+MCQs 1000+ high definition colour clinical photographs and illustrationsFrom EverandThe Unofficial Guide to Paediatrics: Core Curriculum, OSCEs, clinical examinations, practical skills, 60+ clinical cases, 200+MCQs 1000+ high definition colour clinical photographs and illustrationsRating: 2.5 out of 5 stars2.5/5 (2)
- International Medical Graduate and the United States Medical Residency Application: A Guide to Achieving SuccessFrom EverandInternational Medical Graduate and the United States Medical Residency Application: A Guide to Achieving SuccessRaghav GovindarajanNo ratings yet
- 1D2018 - Merit List PDFDocument487 pages1D2018 - Merit List PDFKamran MallickNo ratings yet
- EntDocument1 pageEntKamran MallickNo ratings yet
- ChallanDocument1 pageChallanKamran MallickNo ratings yet
- General Surgery NuggetsDocument12 pagesGeneral Surgery Nuggetsamna_badar1No ratings yet
- Final Year Solved Papers: Athar AliDocument10 pagesFinal Year Solved Papers: Athar AlidrusmansaleemNo ratings yet
- Med-Com's Clinical ReviewDocument7 pagesMed-Com's Clinical Reviewkamran_zarrarNo ratings yet
- List of DMG Officers Posted in The PunjabDocument33 pagesList of DMG Officers Posted in The PunjabKamran MallickNo ratings yet
- Ortho and Salivary Gland Tumor GuideDocument16 pagesOrtho and Salivary Gland Tumor GuideKamran MallickNo ratings yet
- Kod Final YearDocument40 pagesKod Final YearKamran MallickNo ratings yet
- Topics You Cant Afford To Miss in Community MedicineDocument4 pagesTopics You Cant Afford To Miss in Community MedicineKamran MallickNo ratings yet
- Gynecology 2013 KeyDocument4 pagesGynecology 2013 KeyKamran MallickNo ratings yet
- MCQ Paediatrics Group 2Document4 pagesMCQ Paediatrics Group 2Rajiv KabadNo ratings yet
- 01 Aimc 2016Document38 pages01 Aimc 2016Kamran MallickNo ratings yet
- 3 (15 Files Merged)Document15 pages3 (15 Files Merged)Kamran MallickNo ratings yet
- A Final Year Medical Student - SEEKDocument58 pagesA Final Year Medical Student - SEEKKamran MallickNo ratings yet
- Laanti InsanDocument1 pageLaanti InsanKamran MallickNo ratings yet
- Amir Khusro..... PoetryDocument10 pagesAmir Khusro..... PoetrymohammedanwaarNo ratings yet
- Dil-e-Wehshi by Ibn-e-InshaDocument126 pagesDil-e-Wehshi by Ibn-e-Inshaheera100% (2)
- NucleotidesDocument1 pageNucleotidesKamran MallickNo ratings yet
- List of Candidates Selected for Ameer ud Din Medical College Lahore Session 2016-2017Document13 pagesList of Candidates Selected for Ameer ud Din Medical College Lahore Session 2016-2017Kamran MallickNo ratings yet
- Send Up PDFDocument1 pageSend Up PDFKamran MallickNo ratings yet
- UKDocument5 pagesUKkamran_zarrarNo ratings yet
- Exhibit 1 18 116 PDFDocument27 pagesExhibit 1 18 116 PDFSimonNo ratings yet
- Business-Process Integration: Supply-Chain Management 2.0 (SCM 2.0)Document8 pagesBusiness-Process Integration: Supply-Chain Management 2.0 (SCM 2.0)nidayousafzaiNo ratings yet
- Corporate Citizenship, Social Responsibility, Responsiveness, and PerformanceDocument27 pagesCorporate Citizenship, Social Responsibility, Responsiveness, and Performanceguru2k9100% (1)
- Build A Tunnel: What You NeedDocument2 pagesBuild A Tunnel: What You NeedManila Business ShopsNo ratings yet
- Grid Infrastructure Installation and Upgrade Guide Ibm Aix Power Systems 64 BitDocument284 pagesGrid Infrastructure Installation and Upgrade Guide Ibm Aix Power Systems 64 BitAntonioNo ratings yet
- Gen-6000-0mh0/0mhe Gen-6000-0mk0 Gen-6000-0ms0/0mse Gen-7500-0mh0/0mhe Gen-8000-0mk0/0mke Gen-8000-0ms0/0mseDocument26 pagesGen-6000-0mh0/0mhe Gen-6000-0mk0 Gen-6000-0ms0/0mse Gen-7500-0mh0/0mhe Gen-8000-0mk0/0mke Gen-8000-0ms0/0mseAhmed Khodja KarimNo ratings yet
- Lecture 8 - Life Cycle Inventory Example and SimaPro Intro - S18Document42 pagesLecture 8 - Life Cycle Inventory Example and SimaPro Intro - S18Francisco AraujoNo ratings yet
- Ratio, Proportion, and Percent: Presented By: John Darryl M. Genio Bocobo #3Document18 pagesRatio, Proportion, and Percent: Presented By: John Darryl M. Genio Bocobo #3John Darryl GenioNo ratings yet
- Quotation For Villa Maintainance at Al RiqqaDocument2 pagesQuotation For Villa Maintainance at Al RiqqaAkosh AchuNo ratings yet
- Cost Accounting DQ - Midterms - AnswersDocument10 pagesCost Accounting DQ - Midterms - AnswersKurt dela TorreNo ratings yet
- Community Health Nursing Family Nursing AssessmentDocument2 pagesCommunity Health Nursing Family Nursing AssessmentRy LlanesNo ratings yet
- Regenerative Braking System: An Efficient Way to Conserve EnergyDocument31 pagesRegenerative Braking System: An Efficient Way to Conserve EnergyPRAVIN KUMAR NNo ratings yet
- SC WD 1 WashHandsFlyerFormatted JacobHahn Report 1Document3 pagesSC WD 1 WashHandsFlyerFormatted JacobHahn Report 1jackson leeNo ratings yet
- Service ManualDocument14 pagesService ManualOlegNo ratings yet
- Porter 5 ForcesDocument44 pagesPorter 5 ForcesSwapnil ChonkarNo ratings yet
- Chapter 2 EnglishDocument9 pagesChapter 2 Englishdgdhdh_66No ratings yet
- Effective Postoperative Pain Management StrategiesDocument10 pagesEffective Postoperative Pain Management StrategiesvenkayammaNo ratings yet
- Dimensions of Comparative EducationDocument5 pagesDimensions of Comparative Educationeminentsurvivor9No ratings yet
- Drift Punch: Product Features ProfilesDocument3 pagesDrift Punch: Product Features ProfilesPutra KurniaNo ratings yet
- CamScanner Scanned PDF DocumentDocument205 pagesCamScanner Scanned PDF DocumentNabila Tsuroya BasyaNo ratings yet
- Project Proposal ApprovedDocument2 pagesProject Proposal ApprovedRonnel BechaydaNo ratings yet
- Sample COBOL ProgramsDocument35 pagesSample COBOL Programsrahul tejNo ratings yet
- J S S 1 Maths 1st Term E-Note 2017Document39 pagesJ S S 1 Maths 1st Term E-Note 2017preciousNo ratings yet
- Grand Central Terminal Mep Handbook 180323Document84 pagesGrand Central Terminal Mep Handbook 180323Pete A100% (1)
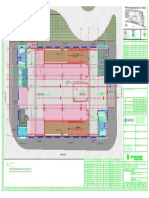
- Key plan and area statement comparison for multi-level car park (MLCPDocument1 pageKey plan and area statement comparison for multi-level car park (MLCP121715502003 BOLLEMPALLI BINDU SREE SATYANo ratings yet
- Examen 03 Aula - F PostgradoDocument5 pagesExamen 03 Aula - F PostgradodiegoNo ratings yet
- Admission Form BA BSC Composite PDFDocument6 pagesAdmission Form BA BSC Composite PDFKhurram ShahzadNo ratings yet
- 04 Vendor Registration TrainingDocument16 pages04 Vendor Registration TrainingAhmad Ramin AbasyNo ratings yet
- Linux Plus Lpi LabsDocument94 pagesLinux Plus Lpi LabsKamib HamibebNo ratings yet
- Installation Guide for lemonPOS POS SoftwareDocument4 pagesInstallation Guide for lemonPOS POS SoftwareHenry HubNo ratings yet