You might also like
- Sensors: Adaptive PIF Control For Permanent Magnet Synchronous Motors Based On GPCDocument18 pagesSensors: Adaptive PIF Control For Permanent Magnet Synchronous Motors Based On GPCebrahimpanNo ratings yet
- Yjmt 23 188Document9 pagesYjmt 23 188ebrahimpanNo ratings yet
- Models For DC MotorsDocument8 pagesModels For DC MotorsebrahimpanNo ratings yet
- Solution 2Document5 pagesSolution 2Paulina MarquezNo ratings yet
- Open Sim Tutorial 1Document10 pagesOpen Sim Tutorial 1Rayanne FlorianoNo ratings yet
- Design and Implementation of A Distributed Variable Impedance Actuator Using Parallel Linear SpringsDocument12 pagesDesign and Implementation of A Distributed Variable Impedance Actuator Using Parallel Linear SpringsebrahimpanNo ratings yet
- c3d2OpenSim TutorialDocument8 pagesc3d2OpenSim Tutorialebrahimpan100% (1)
- Mechatronics: Haoyong Yu, Sunan Huang, Gong Chen, Nitish ThakorDocument12 pagesMechatronics: Haoyong Yu, Sunan Huang, Gong Chen, Nitish ThakorebrahimpanNo ratings yet
- DC motor dynamic modeling and control techniquesDocument23 pagesDC motor dynamic modeling and control techniquesKaderNo ratings yet
- Adaptation of Multijoint Coordination During Standing Balance in Healthy Young and Healthy Old IndividualsDocument14 pagesAdaptation of Multijoint Coordination During Standing Balance in Healthy Young and Healthy Old IndividualsebrahimpanNo ratings yet
- Open Sim Tutorial 1Document10 pagesOpen Sim Tutorial 1Rayanne FlorianoNo ratings yet
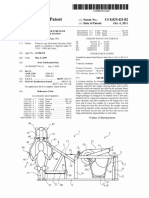
- United States Patent (10) Patent N6 US 8,029,424 B2: Thulin 45 Date of Patent: Oct. 4 2011Document15 pagesUnited States Patent (10) Patent N6 US 8,029,424 B2: Thulin 45 Date of Patent: Oct. 4 2011ebrahimpanNo ratings yet
- 100720141556121410000Document6 pages100720141556121410000ebrahimpanNo ratings yet
- Adaptation of Multijoint Coordination During Standing Balance in Healthy Young and Healthy Old IndividualsDocument14 pagesAdaptation of Multijoint Coordination During Standing Balance in Healthy Young and Healthy Old IndividualsebrahimpanNo ratings yet
- Spring Over Muscle (SOM) Actuator For Rehabilitation DevicesDocument4 pagesSpring Over Muscle (SOM) Actuator For Rehabilitation DevicesebrahimpanNo ratings yet
- An Assisted Waist Supporter For Vertebral RehabilitationDocument2 pagesAn Assisted Waist Supporter For Vertebral RehabilitationebrahimpanNo ratings yet
- I6 BrochureDocument2 pagesI6 BrochureebrahimpanNo ratings yet
- Three-Dimensional Joint Reaction Forces and Moments at The Low Ba PDFDocument9 pagesThree-Dimensional Joint Reaction Forces and Moments at The Low Ba PDFebrahimpanNo ratings yet
- A Review of The Use of Electro-Motor Stimulation in Human MusclesDocument13 pagesA Review of The Use of Electro-Motor Stimulation in Human MusclesebrahimpanNo ratings yet
- A Review of The Clinical Value of Isolated Lumbar Extension Resistance Training For Chronic Low Back PainDocument19 pagesA Review of The Clinical Value of Isolated Lumbar Extension Resistance Training For Chronic Low Back PainebrahimpanNo ratings yet
- 100720141556121410000Document6 pages100720141556121410000ebrahimpanNo ratings yet
- Watanabe 2010Document4 pagesWatanabe 2010ebrahimpanNo ratings yet
- Viscoelasticity - RheologicalDocument10 pagesViscoelasticity - RheologicalsaltyNo ratings yet
- Hasegawa 1985Document6 pagesHasegawa 1985ebrahimpanNo ratings yet
- Supported Contact Mechanics ModelsDocument8 pagesSupported Contact Mechanics ModelsebrahimpanNo ratings yet
- Strain CylindricalDocument4 pagesStrain CylindricalebrahimpanNo ratings yet
- Elastic Constitutive EquationsDocument46 pagesElastic Constitutive EquationsAmithkumar R AchariNo ratings yet
- Mca 21 00016 v2 PDFDocument15 pagesMca 21 00016 v2 PDFebrahimpanNo ratings yet
- Hasegawa 1985Document6 pagesHasegawa 1985ebrahimpanNo ratings yet
- Plane Strain Problems of Transversely Isotropic Thermoelastic MediaDocument15 pagesPlane Strain Problems of Transversely Isotropic Thermoelastic MediaebrahimpanNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Technical Equipment For Assessment of Dental Pulp StatusDocument12 pagesTechnical Equipment For Assessment of Dental Pulp StatusRbk FairladyNo ratings yet
- Multi-Level Skin Resurfacing SystemDocument2 pagesMulti-Level Skin Resurfacing Systemmahmoud mohamedNo ratings yet
- Beck PDFDocument3 pagesBeck PDFfaithnicNo ratings yet
- Complications of General AnesthesiaDocument11 pagesComplications of General AnesthesiaamexatoNo ratings yet
- SOWK3040 Unit3Document19 pagesSOWK3040 Unit3Luckesha ThomasNo ratings yet
- ACLS Test Sinus BradycardiaDocument1 pageACLS Test Sinus BradycardiaFiya Sahrul0% (1)
- What Are Basal and Squamous Cell Skin Cancers?Document13 pagesWhat Are Basal and Squamous Cell Skin Cancers?dodinhtoiNo ratings yet
- LEPROSY, PREGNANCY & TUBERCULOSIS: A REVIEW OF IMPACT AND MANAGEMENTDocument48 pagesLEPROSY, PREGNANCY & TUBERCULOSIS: A REVIEW OF IMPACT AND MANAGEMENTBhawna Joshi100% (1)
- Sleep-Wake Disorders Fact Sheet PDFDocument2 pagesSleep-Wake Disorders Fact Sheet PDFAle M. MartinezNo ratings yet
- 37 - The Five Elements of HomotoxicologyDocument1 page37 - The Five Elements of HomotoxicologyRui PiresNo ratings yet
- MicroCurrent Consent Form 2Document2 pagesMicroCurrent Consent Form 2suniel8080No ratings yet
- Drug Study ParacetamolDocument1 pageDrug Study ParacetamolAbigail Basco100% (2)
- Aged Care Overview BookletDocument88 pagesAged Care Overview BookletABC News OnlineNo ratings yet
- ST John First Aid Course Questions & AnswersDocument3 pagesST John First Aid Course Questions & AnswersJames Hanlon70% (30)
- NU 314 Course Syllabus Spring 2016Document4 pagesNU 314 Course Syllabus Spring 2016Agnes Buñag DoteNo ratings yet
- NSS-12 Ammonium SulfateDocument1 pageNSS-12 Ammonium SulfateMoxzJr VianzNo ratings yet
- Counseling CompilationDocument9 pagesCounseling CompilationEvangeline GuibaoNo ratings yet
- Product Summary FOR Enhanced Hospital & Surgical Insurance AND Group Major Medical InsuranceDocument8 pagesProduct Summary FOR Enhanced Hospital & Surgical Insurance AND Group Major Medical InsuranceAxel KruseNo ratings yet
- Conduction Blocks in AMI: A Prospective StudyDocument6 pagesConduction Blocks in AMI: A Prospective StudyJack JacksonNo ratings yet
- Study Consipation Howaru-TransitDocument8 pagesStudy Consipation Howaru-TransitMộc MộcNo ratings yet
- OB - GYN Clerkship Charts - Google Drive PDFDocument1 pageOB - GYN Clerkship Charts - Google Drive PDFrpascua123No ratings yet
- A Qualitative Exploration of Primary School Students Experience & Utilization of Mindfullness-2017Document14 pagesA Qualitative Exploration of Primary School Students Experience & Utilization of Mindfullness-2017K. KhanNo ratings yet
- 023-Rational Use of DrugsDocument43 pages023-Rational Use of DrugsfikebatuNo ratings yet
- Case Presentation On Autosomal Recessive Polycystic Kidney Disease (ARPKD)Document15 pagesCase Presentation On Autosomal Recessive Polycystic Kidney Disease (ARPKD)narseya100% (1)
- Gastrointestinal BleedingDocument31 pagesGastrointestinal BleedingDenice IsidroNo ratings yet
- Community Health Nursing: Primary Goals and RolesDocument42 pagesCommunity Health Nursing: Primary Goals and RolesChucky VergaraNo ratings yet
- Cannabis ReportDocument7 pagesCannabis ReportKlaudija LutovskaNo ratings yet
- Sikalite: Powdered Waterproofing Admixture For MortarDocument3 pagesSikalite: Powdered Waterproofing Admixture For Mortareye4aneye1989No ratings yet
- Chronic Inflammatory Demyelinating PolyradiculoneuropathyDocument5 pagesChronic Inflammatory Demyelinating PolyradiculoneuropathyDiego Fernando AlegriaNo ratings yet
- Mens Health March 2019 EnglandDocument132 pagesMens Health March 2019 EnglandTigran KarhanyanNo ratings yet