You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Region II Trauma Center Monthly Consumption ReportDocument2 pagesRegion II Trauma Center Monthly Consumption ReportAr JayNo ratings yet
- CSC SPMS PDFDocument56 pagesCSC SPMS PDFAr JayNo ratings yet
- Format of ReportDocument3 pagesFormat of ReportAr JayNo ratings yet
- Course Outline:: Basic Accounting Principles and Financial ConceptsDocument2 pagesCourse Outline:: Basic Accounting Principles and Financial ConceptsAr JayNo ratings yet
- Civil Service VRH Iso Petu: (As Individual Staff Nurse/ Midwife/ Nursing Attendant) (As A Unit/Section/Ward) (As A Nurse)Document1 pageCivil Service VRH Iso Petu: (As Individual Staff Nurse/ Midwife/ Nursing Attendant) (As A Unit/Section/Ward) (As A Nurse)Ar JayNo ratings yet
- List of Quality IndicatorsDocument2 pagesList of Quality IndicatorsAr JayNo ratings yet
- Medical and Office Equipment Fuctionality Monitoring SheetDocument3 pagesMedical and Office Equipment Fuctionality Monitoring SheetAr JayNo ratings yet
- Daily Performance Output ReportDocument5 pagesDaily Performance Output ReportAr JayNo ratings yet
- Medical Supply Monitoring SheetDocument3 pagesMedical Supply Monitoring SheetAr JayNo ratings yet
- Level III Evaluation - Behavioral LevelDocument2 pagesLevel III Evaluation - Behavioral LevelAr JayNo ratings yet
- Form Daily Individual Performance Management ChecklistDocument4 pagesForm Daily Individual Performance Management ChecklistAr JayNo ratings yet
- Com-Spms Form No. 3 (Ipcr) : (Please Add Rows If Necessary)Document3 pagesCom-Spms Form No. 3 (Ipcr) : (Please Add Rows If Necessary)Ar Jay100% (13)
- Emergency Drug Monitoring SheetDocument3 pagesEmergency Drug Monitoring SheetAr JayNo ratings yet
- Census Remark Code Task Q E T: Surgical Intensive Care UnitDocument1 pageCensus Remark Code Task Q E T: Surgical Intensive Care UnitAr JayNo ratings yet
- List of Quality IndicatorsDocument2 pagesList of Quality IndicatorsAr JayNo ratings yet
- CSC SPMS PDFDocument56 pagesCSC SPMS PDFAr JayNo ratings yet
- Department of SurgeryDocument2 pagesDepartment of SurgeryAr Jay100% (1)
- Ipcr Kabisote Ob orDocument2 pagesIpcr Kabisote Ob orAr JayNo ratings yet
- Introductory Article - OPDDocument1 pageIntroductory Article - OPDAr JayNo ratings yet
- Etoshow QuityDocument8 pagesEtoshow QuityAr JayNo ratings yet
- CompetencyDocument7 pagesCompetencyAr JayNo ratings yet
- PArts Please PrintDocument1 pagePArts Please PrintAr JayNo ratings yet
- Quality IndicatorsDocument45 pagesQuality IndicatorsAr JayNo ratings yet
- b1 FinelliDocument42 pagesb1 FinelliAr JayNo ratings yet
- Quality IndicatorsDocument152 pagesQuality IndicatorsAr JayNo ratings yet
- Infection Control RiskDocument2 pagesInfection Control RiskAr JayNo ratings yet
- Surgical Intensive Care Unit-Nuerovital Signs Monitoring ToolDocument1 pageSurgical Intensive Care Unit-Nuerovital Signs Monitoring ToolAr JayNo ratings yet
- Give Psychological Support To The Patient and FamilyDocument2 pagesGive Psychological Support To The Patient and FamilyNílo StárnNo ratings yet
- Assessing A PatientDocument1 pageAssessing A PatientAr JayNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Psycho Physiological Disorders 1Document8 pagesPsycho Physiological Disorders 1Cedric Jay Villegas TasicoNo ratings yet
- Abdominal Pain Case PresentationDocument52 pagesAbdominal Pain Case PresentationNico Avellana100% (1)
- 2020-68 Annex B - Health Declaration Form110320Document4 pages2020-68 Annex B - Health Declaration Form110320Aileen MayaNo ratings yet
- CefaclorDocument3 pagesCefaclorAyah PaasaNo ratings yet
- NCP HeadDocument11 pagesNCP Headann-lisel-manahan-7670100% (2)
- Acupressure Points For Relieving ArthritisDocument18 pagesAcupressure Points For Relieving ArthritisAgustin Benitez Holguin100% (4)
- 2021 - Viral Vector-Based Gene Therapies in The ClinicDocument20 pages2021 - Viral Vector-Based Gene Therapies in The ClinicMaykol Hernán Rojas SánchezNo ratings yet
- Courvosier Law PDFDocument6 pagesCourvosier Law PDFElno TatipikalawanNo ratings yet
- CIDI-based Screening Scale For Bipolar Spectrum Disorders - : Clinical UtilityDocument4 pagesCIDI-based Screening Scale For Bipolar Spectrum Disorders - : Clinical UtilityJagdishVankarNo ratings yet
- Essay 5Document13 pagesEssay 5api-549025764No ratings yet
- Diazoxide 50mg Tab DCC SummeryDocument1 pageDiazoxide 50mg Tab DCC SummeryarifpharmjuNo ratings yet
- PERKENI (2021) - Konsensus DM Tipe 2Document119 pagesPERKENI (2021) - Konsensus DM Tipe 2Ammalia RachmiNo ratings yet
- Diabetic Ketoacidosis in ChildrenDocument39 pagesDiabetic Ketoacidosis in ChildrenRichard SiahaanNo ratings yet
- Tif30Document49 pagesTif30HCX dghhqNo ratings yet
- Acute GastroenteritisDocument48 pagesAcute Gastroenteritisansam kamalNo ratings yet
- Post-Op OliguriaDocument13 pagesPost-Op OliguriaNigel SparksNo ratings yet
- Gynecology GY Emtyaz Quiz JordanDocument40 pagesGynecology GY Emtyaz Quiz JordanVicviclookThekingNo ratings yet
- Classification of Endometriosis: Birmingham, AlabamaDocument2 pagesClassification of Endometriosis: Birmingham, AlabamaAsela SubhasingheNo ratings yet
- Understanding Thrombophilia Risk FactorsDocument9 pagesUnderstanding Thrombophilia Risk FactorsSeraj Abed ElmoatiNo ratings yet
- Case Presentation-Nasopharyngeal CarcinomaDocument18 pagesCase Presentation-Nasopharyngeal Carcinomatehkie04100% (3)
- Sir 2Document5 pagesSir 2Patziedawn GonzalvoNo ratings yet
- Breast - Calcifications Differential Diagnosis: Anatomy Diagnostic ApproachDocument22 pagesBreast - Calcifications Differential Diagnosis: Anatomy Diagnostic ApproachDokdem AjaNo ratings yet
- Drug StudyDocument1 pageDrug StudyJeremiah M. MascariñasNo ratings yet
- Fisa de Disciplina - ENG - Reumatologie - 2019 - 2020Document4 pagesFisa de Disciplina - ENG - Reumatologie - 2019 - 2020flo108No ratings yet
- Faktor-Faktor Yang Mempengaruhi Gangguan Tidur Pada Pasien Diabetes MelitusDocument6 pagesFaktor-Faktor Yang Mempengaruhi Gangguan Tidur Pada Pasien Diabetes MelitusImron BuhoriNo ratings yet
- Graduate SOAP NOTE TEMPLATEDocument7 pagesGraduate SOAP NOTE TEMPLATEMiley MunozNo ratings yet
- Gastroesophageal Reflux Disease (Gerd) : By: Therese Jane TimbalopezDocument14 pagesGastroesophageal Reflux Disease (Gerd) : By: Therese Jane Timbalopezjoyrena ochondraNo ratings yet
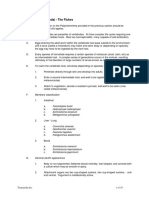
- Class Digenea (Trematoda) - The FlukesDocument10 pagesClass Digenea (Trematoda) - The FlukesAmr EldemardashNo ratings yet
- Gold Standards in Medical FieldDocument8 pagesGold Standards in Medical FieldJyothisankar Radhakrishnan100% (2)
- Matrix Viscoelasticity Promotes Liver Cancer Progression in The Pre-Cirrhotic LiverDocument31 pagesMatrix Viscoelasticity Promotes Liver Cancer Progression in The Pre-Cirrhotic LiverinfoNo ratings yet