You might also like
- Ultrasound Predictors of Placental Invasion: The Placenta Accreta IndexDocument7 pagesUltrasound Predictors of Placental Invasion: The Placenta Accreta IndexMarendra MahathirNo ratings yet
- The "Rail Sign": An Ultrasound Finding in Placenta Accreta Spectrum Indicating Deep Villous Invasion and Adverse OutcomesDocument17 pagesThe "Rail Sign": An Ultrasound Finding in Placenta Accreta Spectrum Indicating Deep Villous Invasion and Adverse OutcomesJoseLuisNo ratings yet
- Ultrasound Prediction of Placenta Accreta AccuracyDocument7 pagesUltrasound Prediction of Placenta Accreta AccuracyRaisa AriesthaNo ratings yet
- P ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Document2 pagesP ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)shelly_shellyNo ratings yet
- Grayscale USG of Placenta AccretaDocument5 pagesGrayscale USG of Placenta AccretaDara Mayang SariNo ratings yet
- Placenta Previa: Distance To Internal Os and Mode of DeliveryDocument3 pagesPlacenta Previa: Distance To Internal Os and Mode of DeliveryZEMENAY TRUNEHNo ratings yet
- Screening For Placenta Accreta at 11-14 Weeks of GestationDocument6 pagesScreening For Placenta Accreta at 11-14 Weeks of Gestationjuljim01No ratings yet
- Committee Opinion: Placenta AccretaDocument5 pagesCommittee Opinion: Placenta AccretaagungNo ratings yet
- Jurnal Plasenta Akreta PDFDocument5 pagesJurnal Plasenta Akreta PDFfatqur28No ratings yet
- Diagnosis and Management of PlacentaDocument16 pagesDiagnosis and Management of PlacentaYoga ParipurnaNo ratings yet
- Jurnal Bhs. Inggris Obgyn 1Document7 pagesJurnal Bhs. Inggris Obgyn 1RiLa Dwi KurniatiNo ratings yet
- Gray Scale and Doppler Ultrasound in Placenta AccrDocument5 pagesGray Scale and Doppler Ultrasound in Placenta AccrRicky JunaediNo ratings yet
- Prediction of Morbidly Adherent Placenta Using A Scoring SystemDocument7 pagesPrediction of Morbidly Adherent Placenta Using A Scoring SystemClaudio UdjajaNo ratings yet
- Clinical and Ultrasound Assessment in Patients WitDocument8 pagesClinical and Ultrasound Assessment in Patients Witrk vNo ratings yet
- Prenatal DiagnosisDocument8 pagesPrenatal DiagnosisEstefania GutierrezNo ratings yet
- Diagnosis and Management of Isthmocele (Cesarean Scar Defect) A SWOT AnalysisDocument9 pagesDiagnosis and Management of Isthmocele (Cesarean Scar Defect) A SWOT AnalysisWillans Eduardo Rosha HumerezNo ratings yet
- Natural History of Vasa Previa Across Gestation Using A Screening ProtocolDocument7 pagesNatural History of Vasa Previa Across Gestation Using A Screening ProtocolwijeNo ratings yet
- Ultrasound in Obstet Gyne - 2021 - Skupski - Evaluation of Classic and Novel Ultrasound Signs of Placenta AccretaDocument9 pagesUltrasound in Obstet Gyne - 2021 - Skupski - Evaluation of Classic and Novel Ultrasound Signs of Placenta AccretaVeronica Suárez Baldeón100% (1)
- Ultrasound in Obstet Gyne - 2013 - Kok - Sonographic Measurement of Lower Uterine Segment Thickness To Predict UterineDocument8 pagesUltrasound in Obstet Gyne - 2013 - Kok - Sonographic Measurement of Lower Uterine Segment Thickness To Predict UterineObsgin Januari17No ratings yet
- Ajog 2Document6 pagesAjog 2Coc OfclansNo ratings yet
- Ultrasound in Obstet Gyne - 2006 - Yang - Sonographic Findings of Placental Lacunae and The Prediction of AdherentDocument5 pagesUltrasound in Obstet Gyne - 2006 - Yang - Sonographic Findings of Placental Lacunae and The Prediction of AdherentdanielNo ratings yet
- Committee Opinion: Placenta AccretaDocument5 pagesCommittee Opinion: Placenta AccretabebetteryesyoucanNo ratings yet
- Placenta Accreta, Increta and PercretaDocument18 pagesPlacenta Accreta, Increta and Percretarutsanchez01No ratings yet
- Risk Factors For Umbilical Cord Prolapse at The Time of Arti Ficial Rupture of MembranesDocument6 pagesRisk Factors For Umbilical Cord Prolapse at The Time of Arti Ficial Rupture of MembranesElva Diany SyamsudinNo ratings yet
- 11 Abnormal PlacentationDocument29 pages11 Abnormal PlacentationMaria Gabriela CristanchoNo ratings yet
- Frequency of Morbidly Adherent Placenta in Previous Scar: Fakhar Un Nissa, Saira Dars, Shazia Awan, Firdous MumtazDocument5 pagesFrequency of Morbidly Adherent Placenta in Previous Scar: Fakhar Un Nissa, Saira Dars, Shazia Awan, Firdous MumtazprobouNo ratings yet
- BJMG 20 005 PDFDocument5 pagesBJMG 20 005 PDFRakka Fawwaz IlhamNo ratings yet
- Placenta Accreta Spectrum and Postpartum Hemorrhag - 230510 - 170158Document10 pagesPlacenta Accreta Spectrum and Postpartum Hemorrhag - 230510 - 170158Nilfacio PradoNo ratings yet
- Placenta Accreta A Practical Review 2020Document6 pagesPlacenta Accreta A Practical Review 2020Adriana MartínezNo ratings yet
- Acretismo PlacentarioDocument9 pagesAcretismo PlacentarioRolando LaraNo ratings yet
- ACOG Guides and Opinion On Placenta Accreta ManagementDocument5 pagesACOG Guides and Opinion On Placenta Accreta ManagementCharlene FernándezNo ratings yet
- Piis0002937812004024 PDFDocument13 pagesPiis0002937812004024 PDFYusufNo ratings yet
- The Placenta Accreta Spectrum: Pathophysiology and Evidence-Based Anatomy For Prenatal Ultrasound ImagingDocument14 pagesThe Placenta Accreta Spectrum: Pathophysiology and Evidence-Based Anatomy For Prenatal Ultrasound ImagingIriamana Liasyarah MarudinNo ratings yet
- Jurnal Obgyn 2018 2Document15 pagesJurnal Obgyn 2018 2aulNo ratings yet
- Placenta PercretaDocument8 pagesPlacenta PercretaBrigitte GutierrezNo ratings yet
- Cesarean Scar Ectopic Pregnancies: Etiology, Diagnosis, and ManagementDocument9 pagesCesarean Scar Ectopic Pregnancies: Etiology, Diagnosis, and ManagementDinorah MarcelaNo ratings yet
- Print 1 FixDocument10 pagesPrint 1 Fixafriskha bulawanNo ratings yet
- 2021 Article 1541Document6 pages2021 Article 1541bintangNo ratings yet
- Vasa PraeviaDocument2 pagesVasa PraeviaReinaldo AbenteNo ratings yet
- Early Accreta and Uterine Rupture in The Second Trimester: Open Access Case DOI: 10.7759/cureus.2904Document11 pagesEarly Accreta and Uterine Rupture in The Second Trimester: Open Access Case DOI: 10.7759/cureus.2904Iqbal LambaraNo ratings yet
- Ultrasonographic Prediction of Placental Invasion in Placenta Previa by Placenta Accreta IndexDocument8 pagesUltrasonographic Prediction of Placental Invasion in Placenta Previa by Placenta Accreta IndexMuh AqwilNo ratings yet
- Maternal and Foetal Outcomes of Cesarean Hysterectomies for Placenta IncretaDocument3 pagesMaternal and Foetal Outcomes of Cesarean Hysterectomies for Placenta IncretaNununkNo ratings yet
- FIGO Accreta Prenantal DiagnosisDocument7 pagesFIGO Accreta Prenantal DiagnosisYosef Dwi Cahyadi SalanNo ratings yet
- Water Imaging FetusDocument9 pagesWater Imaging FetusAndy XiaoNo ratings yet
- Indications and Risks of Vacuum Assisted Deliveries.: OriginalDocument2 pagesIndications and Risks of Vacuum Assisted Deliveries.: OriginalgagagigoNo ratings yet
- Pos Ok Hova 2012Document1 pagePos Ok Hova 2012Suis MionooNo ratings yet
- Cesarean Scar Defect: A Prospective Study On Risk Factors: GynecologyDocument8 pagesCesarean Scar Defect: A Prospective Study On Risk Factors: Gynecologynuphie_nuphNo ratings yet
- Diagnostic Parameters To Differentiate Benign From Malignant Ovarian Masses With Contrast-Enhanced Transvaginal SonographyDocument8 pagesDiagnostic Parameters To Differentiate Benign From Malignant Ovarian Masses With Contrast-Enhanced Transvaginal SonographyRush32No ratings yet
- Sonographic Prediction of Outcome of Vacuum Deliveries: A Multicenter, Prospective Cohort StudyDocument10 pagesSonographic Prediction of Outcome of Vacuum Deliveries: A Multicenter, Prospective Cohort Studysuyudi kimikoNo ratings yet
- Uterine Sutures at Prior Caesarean Section and Placenta Accreta in Subsequent Pregnancy: A Case - Control StudyDocument10 pagesUterine Sutures at Prior Caesarean Section and Placenta Accreta in Subsequent Pregnancy: A Case - Control StudyIsmul 'D' SadlyNo ratings yet
- Good18.Prenatally Diagnosed Vasa Previa A.30Document9 pagesGood18.Prenatally Diagnosed Vasa Previa A.30wije0% (1)
- Poster 2Document1 pagePoster 2cringu.ionescuNo ratings yet
- Silver 2015Document15 pagesSilver 2015Farlinda AlyaNo ratings yet
- Articulo 8Document15 pagesArticulo 8Monica ReyesNo ratings yet
- Eco Intraparto. Cesarea VS VaginalDocument18 pagesEco Intraparto. Cesarea VS VaginalVictor Manuel Restrepo PosadaNo ratings yet
- Prenatal Diagnosis of Congenital Epulis: Implications For DeliveryDocument3 pagesPrenatal Diagnosis of Congenital Epulis: Implications For DeliveryRiznasyarielia Nikmatun NafisahNo ratings yet
- Simcox 2009Document6 pagesSimcox 2009Aulya ArchuletaNo ratings yet
- Placenta Previa 1Document2 pagesPlacenta Previa 1Gunther MirandaNo ratings yet
- Radiology RadiologyDocument6 pagesRadiology RadiologyJonathan ReinaldoNo ratings yet
- Lower Genital Tract Precancer: Colposcopy, Pathology and TreatmentFrom EverandLower Genital Tract Precancer: Colposcopy, Pathology and TreatmentNo ratings yet
- Amenorrhea WilliamsDocument26 pagesAmenorrhea WilliamsGregorius Juan GunawanNo ratings yet
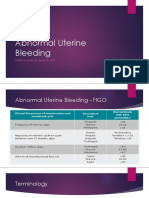
- Abnormal Uterine BleedingDocument33 pagesAbnormal Uterine BleedingGregorius Juan GunawanNo ratings yet
- ACGGuideline Liver Disease and Pregnancy 2016 PDFDocument19 pagesACGGuideline Liver Disease and Pregnancy 2016 PDFArnella HutagalungNo ratings yet
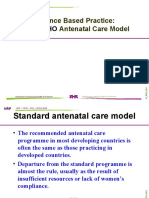
- Evidence Based Practice: A Antenatal Care Model: New WHODocument18 pagesEvidence Based Practice: A Antenatal Care Model: New WHOGregorius Juan GunawanNo ratings yet
- Placenta Acreta IndexDocument13 pagesPlacenta Acreta IndexGregorius Juan GunawanNo ratings yet
- The Anaemia Plasmodium VivaxDocument14 pagesThe Anaemia Plasmodium VivaxDewi Masyithah DarlanNo ratings yet
- Kantin FileDocument1 pageKantin FileGregorius Juan GunawanNo ratings yet
- Carotid and Vertebral Ultrasonography - Dr. DanielDocument74 pagesCarotid and Vertebral Ultrasonography - Dr. DanielSuci Rahayu Evasha100% (1)
- Nicole Wolcott - ResumeDocument3 pagesNicole Wolcott - Resumeapi-308666807No ratings yet
- Acuson nx3 Series Urology Flyer 04919911Document4 pagesAcuson nx3 Series Urology Flyer 04919911Orlando CantilloNo ratings yet
- Siemens Acuson Sc2000 Transducer LiteDocument10 pagesSiemens Acuson Sc2000 Transducer Litebashir019No ratings yet
- Overview of Ophthalmic EquipmentDocument57 pagesOverview of Ophthalmic EquipmentAl RaNo ratings yet
- Innovation And Compact Ultrasound System A Real Game-ChangerDocument4 pagesInnovation And Compact Ultrasound System A Real Game-Changerjuank_m10No ratings yet
- Pregnancy DiagnosisDocument28 pagesPregnancy Diagnosisamit vishenNo ratings yet
- Ankle Brachial Index PDFDocument8 pagesAnkle Brachial Index PDFIncredibleNo ratings yet
- GuideDocument52 pagesGuidemihaelklajner100% (1)
- Epiq 7Document46 pagesEpiq 7Alberto Michielon100% (1)
- Doppler Ultrasound of The KidneysDocument23 pagesDoppler Ultrasound of The KidneysivoklarinNo ratings yet
- Practical EXamDocument5 pagesPractical EXamNDTInstructor100% (6)
- Pulmonary EmbolismDocument53 pagesPulmonary EmbolismSultan Al-rabeahNo ratings yet
- Revision History and SpecificationsDocument304 pagesRevision History and SpecificationsSyarif AlfathNo ratings yet
- Imaging of The Male Reproductive Tract 2020Document8 pagesImaging of The Male Reproductive Tract 2020zulfikarfsnNo ratings yet
- 1 Role of Ultrasound in The Evaluation of Acute Pelvic PainDocument11 pages1 Role of Ultrasound in The Evaluation of Acute Pelvic PainGhofran Ibrahim HassanNo ratings yet
- Medical ImagingDocument12 pagesMedical ImagingKeanan WongsoNo ratings yet
- 2016.11.30 Guidelines Revision1 Final 0Document126 pages2016.11.30 Guidelines Revision1 Final 0Erika KennedyNo ratings yet
- Theriogenology: Elaine M.U. Gil, Daniela A.A. Garcia, Tilde R. FroesDocument6 pagesTheriogenology: Elaine M.U. Gil, Daniela A.A. Garcia, Tilde R. FroesIngrid MachadoNo ratings yet
- EVIS EXERA III BF Concept Brochure 001 v1 GB 20120418Document7 pagesEVIS EXERA III BF Concept Brochure 001 v1 GB 20120418Vera Andri YaniNo ratings yet
- LOGIQ F8 DatasheetDocument12 pagesLOGIQ F8 DatasheetElies67% (3)
- Vision of A New DimensionDocument8 pagesVision of A New DimensionRirin Dwi LestariNo ratings yet
- Ultrasound To GoDocument16 pagesUltrasound To GonanoteraCHNo ratings yet
- Point-Of-Care Ultrasonography For ObstetricsDocument22 pagesPoint-Of-Care Ultrasonography For Obstetricssalah subbahNo ratings yet
- Quisted en P Menopausicas Guias GTG - 34 PDFDocument32 pagesQuisted en P Menopausicas Guias GTG - 34 PDFAdela Marìa P LNo ratings yet
- SelfDirectedLearning CUSScan On NICUDocument43 pagesSelfDirectedLearning CUSScan On NICUmadimadi11No ratings yet
- Clinical Doppler Ultrasound PDFDocument359 pagesClinical Doppler Ultrasound PDFShashi Rajashekar Swamy100% (3)
- Diseases of The SmalllntestineDocument183 pagesDiseases of The SmalllntestineIgor CemortanNo ratings yet
- 3 Tools For Troubleshooting Philips X5-1 Performance IssuesDocument4 pages3 Tools For Troubleshooting Philips X5-1 Performance IssuesMiranda Orozco100% (1)
- Breast Imaging: - DR Anamika Jha, MDDocument122 pagesBreast Imaging: - DR Anamika Jha, MDDr KhanNo ratings yet