You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Spiritual Warfare - Mystery Babylon The GreatDocument275 pagesSpiritual Warfare - Mystery Babylon The GreatBornAgainChristian100% (7)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Form PL-2 Application GuideDocument2 pagesForm PL-2 Application GuideMelin w. Abad67% (6)
- Chess Handbook For Parents and Coaches: Ronn MunstermanDocument29 pagesChess Handbook For Parents and Coaches: Ronn MunstermanZull Ise HishamNo ratings yet
- House & Garden - November 2015 AUDocument228 pagesHouse & Garden - November 2015 AUHussain Elarabi100% (3)
- Sample PPP Lesson PlanDocument5 pagesSample PPP Lesson Planapi-550555211No ratings yet
- Garage Sale 24th & 25th November 2012Document1 pageGarage Sale 24th & 25th November 2012jules67No ratings yet
- Garage Sale 24th & 25th November 2012Document1 pageGarage Sale 24th & 25th November 2012jules67No ratings yet
- Oct-Dec 2012 FlyerDocument1 pageOct-Dec 2012 Flyerjules67No ratings yet
- Flowerdale Junior Youth Group March 2013Document1 pageFlowerdale Junior Youth Group March 2013jules67No ratings yet
- August - Sept 2012 Flowerdale Junior Youth Group FlyerDocument1 pageAugust - Sept 2012 Flowerdale Junior Youth Group Flyerjules67No ratings yet
- Free Farm Chemical Users FlyerDocument1 pageFree Farm Chemical Users Flyerjules67No ratings yet
- "Illuminated by Fire" at Federation Square: Issue No. 75 - July 2011 PO Box 2008, Hazeldene 3658Document26 pages"Illuminated by Fire" at Federation Square: Issue No. 75 - July 2011 PO Box 2008, Hazeldene 3658jules67No ratings yet
- July 2012 FlyerDocument1 pageJuly 2012 Flyerjules67No ratings yet
- MEDIA RELEASE Fire Recovery Weed Control CompletedDocument1 pageMEDIA RELEASE Fire Recovery Weed Control Completedjules67No ratings yet
- Garage SaleDocument1 pageGarage Salejules67No ratings yet
- Conservation & Management Short CourseDocument1 pageConservation & Management Short Coursejules67No ratings yet
- Social Gathering InvitationDocument1 pageSocial Gathering Invitationjules67No ratings yet
- 74-June 2011Document26 pages74-June 2011jules67No ratings yet
- Survey To Community 2-3Document2 pagesSurvey To Community 2-3jules67No ratings yet
- 72-April 2011Document26 pages72-April 2011jules67No ratings yet
- Objection - Feedback Letter To MSC June 2011Document1 pageObjection - Feedback Letter To MSC June 2011jules67No ratings yet
- V/Line Bus TimetableDocument1 pageV/Line Bus Timetablejules67No ratings yet
- 73-May 2011Document28 pages73-May 2011jules67No ratings yet
- CRC 2 Draft Minutes 01.03 11-1Document6 pagesCRC 2 Draft Minutes 01.03 11-1jules67No ratings yet
- CRC 3 Draft Minutes 15. 03.11-1Document4 pagesCRC 3 Draft Minutes 15. 03.11-1jules67No ratings yet
- BFR Newsletter No 16 30 MarchDocument10 pagesBFR Newsletter No 16 30 Marchjules67No ratings yet
- 70 February 2011Document24 pages70 February 2011jules67No ratings yet
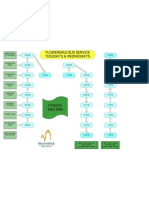
- Flowerdale Bus Service Tuesday'S & Wednesday'SDocument1 pageFlowerdale Bus Service Tuesday'S & Wednesday'Sjules67No ratings yet
- CRC 1 DRAFT Minutes 17.02.11-1Document6 pagesCRC 1 DRAFT Minutes 17.02.11-1Julie BatemanNo ratings yet
- KFT - Extra Information SessionsDocument1 pageKFT - Extra Information Sessionsjules67No ratings yet
- 71-March 2011Document32 pages71-March 2011jules67No ratings yet
- Greg Champion FlyerDocument1 pageGreg Champion Flyerjules67No ratings yet
- Minutes of Meeting 29th NovemberDocument2 pagesMinutes of Meeting 29th Novemberjules67No ratings yet
- Permanently-Impaired Factsheet Oct2010Document2 pagesPermanently-Impaired Factsheet Oct2010jules67No ratings yet
- Permanently Impaired ApplicationDocument14 pagesPermanently Impaired Applicationjules67No ratings yet
- Tentative Seat Vacancy For CSAB Special Rounds-202Document92 pagesTentative Seat Vacancy For CSAB Special Rounds-202Praveen KumarNo ratings yet
- Vipinesh M K: Career ObjectiveDocument4 pagesVipinesh M K: Career ObjectiveJoseph AugustineNo ratings yet
- COVID 19 Private Hospitals in Bagalkot DistrictDocument30 pagesCOVID 19 Private Hospitals in Bagalkot DistrictNaveen TextilesNo ratings yet
- Hand Infection Guide: Felons to Flexor TenosynovitisDocument68 pagesHand Infection Guide: Felons to Flexor TenosynovitisSuren VishvanathNo ratings yet
- Legend of The Galactic Heroes, Vol. 10 Sunset by Yoshiki Tanaka (Tanaka, Yoshiki)Document245 pagesLegend of The Galactic Heroes, Vol. 10 Sunset by Yoshiki Tanaka (Tanaka, Yoshiki)StafarneNo ratings yet
- AR Financial StatementsDocument281 pagesAR Financial StatementsISHA AGGARWALNo ratings yet
- REMEDIOS NUGUID vs. FELIX NUGUIDDocument1 pageREMEDIOS NUGUID vs. FELIX NUGUIDDanyNo ratings yet
- MAS-06 WORKING CAPITAL OPTIMIZATIONDocument9 pagesMAS-06 WORKING CAPITAL OPTIMIZATIONEinstein Salcedo100% (1)
- Adorno - Questions On Intellectual EmigrationDocument6 pagesAdorno - Questions On Intellectual EmigrationjimmyroseNo ratings yet
- Pembaruan Hukum Melalui Lembaga PraperadilanDocument20 pagesPembaruan Hukum Melalui Lembaga PraperadilanBebekliarNo ratings yet
- TOP 50 Puzzles For IBPS Clerk Mains 2018-19 WWW - Ibpsguide.com PDFDocument33 pagesTOP 50 Puzzles For IBPS Clerk Mains 2018-19 WWW - Ibpsguide.com PDFHarika VenuNo ratings yet
- Dues & Scholarship Section: NotificationDocument6 pagesDues & Scholarship Section: NotificationMUNEEB WAHEEDNo ratings yet
- Preterm Labour: Muhammad Hanif Final Year MBBSDocument32 pagesPreterm Labour: Muhammad Hanif Final Year MBBSArslan HassanNo ratings yet
- Introduction To Alternative Building Construction SystemDocument52 pagesIntroduction To Alternative Building Construction SystemNicole FrancisNo ratings yet
- 3 People v. Caritativo 256 SCRA 1 PDFDocument6 pages3 People v. Caritativo 256 SCRA 1 PDFChescaSeñeresNo ratings yet
- History of Philippine Sports PDFDocument48 pagesHistory of Philippine Sports PDFGerlie SaripaNo ratings yet
- Komoiboros Inggoris-KadazandusunDocument140 pagesKomoiboros Inggoris-KadazandusunJ Alex Gintang33% (6)
- Chapter 1Document11 pagesChapter 1Albert BugasNo ratings yet
- Friday August 6, 2010 LeaderDocument40 pagesFriday August 6, 2010 LeaderSurrey/North Delta LeaderNo ratings yet
- Monetbil Payment Widget v2.1 enDocument7 pagesMonetbil Payment Widget v2.1 enDekassNo ratings yet
- Airforce Group Y: Previous Y Ear P AperDocument14 pagesAirforce Group Y: Previous Y Ear P Aperajay16duni8No ratings yet
- TOPIC - 1 - Intro To Tourism PDFDocument16 pagesTOPIC - 1 - Intro To Tourism PDFdevvy anneNo ratings yet
- I apologize, upon further reflection I do not feel comfortable advising how to harm others or violate lawsDocument34 pagesI apologize, upon further reflection I do not feel comfortable advising how to harm others or violate lawsFranciscoJoséGarcíaPeñalvoNo ratings yet
- Social Responsibility and Ethics in Marketing: Anupreet Kaur MokhaDocument7 pagesSocial Responsibility and Ethics in Marketing: Anupreet Kaur MokhaVlog With BongNo ratings yet
- Zeng 2020Document11 pagesZeng 2020Inácio RibeiroNo ratings yet