You might also like
- CPH Lab Activity 7: Automated HematologyDocument44 pagesCPH Lab Activity 7: Automated HematologyChelsea Padilla Delos Reyes100% (1)
- Platelet Count ManualDocument2 pagesPlatelet Count ManualAli Ahmad Khameini100% (1)
- HLG Automata 150428233016 Conversion Gate02Document111 pagesHLG Automata 150428233016 Conversion Gate02Starks Gazer100% (1)
- Blood Morphometry or Blood Film CommentDocument103 pagesBlood Morphometry or Blood Film CommentYangnuu TitusNo ratings yet
- XN Series: Case InterpretationDocument41 pagesXN Series: Case InterpretationTanveerNo ratings yet
- Targeted Cancer TherapyDocument447 pagesTargeted Cancer Therapyivsson100% (1)
- Manual CBC 1 3: - Wbcs - Platelets Count - PCV or HCT - Retics Count - HB Estimation 3 3 4 5 6Document25 pagesManual CBC 1 3: - Wbcs - Platelets Count - PCV or HCT - Retics Count - HB Estimation 3 3 4 5 6Aqila MumtazNo ratings yet
- Flagging and Result Interpretation-1Document41 pagesFlagging and Result Interpretation-1Rini WidyantariNo ratings yet
- BC-6800 Auto Hematology Analyzer Small Cube, Big DifferenceDocument16 pagesBC-6800 Auto Hematology Analyzer Small Cube, Big DifferencePieter Du Toit-EnslinNo ratings yet
- Complete Blood Count GuideDocument20 pagesComplete Blood Count GuideAnastasia100% (1)
- The PCM International Edition v1 Interactive PDFDocument111 pagesThe PCM International Edition v1 Interactive PDFDaniel Augusto Buendia GómezNo ratings yet
- Learning HematologyDocument60 pagesLearning HematologyGiancarlo Doria100% (14)
- Validation Cell AnalyzersDocument45 pagesValidation Cell AnalyzerscandiddreamsNo ratings yet
- Step 2 CK Review - HematologyDocument18 pagesStep 2 CK Review - Hematologyrsmd1986No ratings yet
- Platelet CountDocument2 pagesPlatelet CountSirias_black100% (2)
- Using Hematology Data to Solve Medical MysteriesDocument82 pagesUsing Hematology Data to Solve Medical MysteriesSai Kumar KonukuNo ratings yet
- Good CBC Principle, Interpretation PDFDocument47 pagesGood CBC Principle, Interpretation PDFARIF AHAMMED P100% (1)
- Oncologic NursingDocument132 pagesOncologic Nursingɹǝʍdןnos100% (10)
- Basic HematologyDocument89 pagesBasic Hematologydrafq2000No ratings yet
- Hematology 2Document58 pagesHematology 2Laboratorium Ansari SalehNo ratings yet
- HCV diagnostic and health care worker managementDocument36 pagesHCV diagnostic and health care worker managementLaboratorium Ansari SalehNo ratings yet
- Med Surg Chapters 19 - 20 Hematologic Functions and Disorders PPT and QuestionsDocument36 pagesMed Surg Chapters 19 - 20 Hematologic Functions and Disorders PPT and QuestionsAshley100% (1)
- Platelet Counts: Historical Perspectives and Case StudiesDocument35 pagesPlatelet Counts: Historical Perspectives and Case Studiesshikhar623No ratings yet
- Hematology 3Document22 pagesHematology 3Laboratorium Ansari SalehNo ratings yet
- Result Interpretation: Flags, Masks, Messages & RBC/PLT AnalysisDocument63 pagesResult Interpretation: Flags, Masks, Messages & RBC/PLT AnalysisMarcellia Angelina100% (1)
- Part 1 Haematology Examination: Multiple Choice QuestionsDocument9 pagesPart 1 Haematology Examination: Multiple Choice Questionsmma1976100% (1)
- Immunologi 2Document44 pagesImmunologi 2Laboratorium Ansari SalehNo ratings yet
- Fast Facts: CAR T-Cell Therapy in Diffuse Large B-Cell Lymphoma: A practical resource for nursesFrom EverandFast Facts: CAR T-Cell Therapy in Diffuse Large B-Cell Lymphoma: A practical resource for nursesNo ratings yet
- Clinical Case Report - XS-1000i - SpanishDocument45 pagesClinical Case Report - XS-1000i - SpanishLaboratorios Clinicos ZaragozaNo ratings yet
- Pembacaan Histogram Dan Scattergram Pada Hematologi Analyzer IraDocument36 pagesPembacaan Histogram Dan Scattergram Pada Hematologi Analyzer Irairaawatii80% (5)
- Diagnosis Dan Tatalaksana Tuberkulosis: Dr. DR Erlina Burhan Msc. SP.P (K)Document44 pagesDiagnosis Dan Tatalaksana Tuberkulosis: Dr. DR Erlina Burhan Msc. SP.P (K)Laboratorium Ansari SalehNo ratings yet
- Automated Hematology Analyzer: Presenter: DR - KeerthyDocument95 pagesAutomated Hematology Analyzer: Presenter: DR - KeerthyadiNo ratings yet
- 2-DxH Case BookDocument56 pages2-DxH Case BookOm PrakashNo ratings yet
- Interpretation of HistogramDocument92 pagesInterpretation of HistogramJagu ShahNo ratings yet
- General IntroductionDocument9 pagesGeneral IntroductionCuong VuNo ratings yet
- DR Preeti Mansukhani - CBC 5 Parts - 2017Document56 pagesDR Preeti Mansukhani - CBC 5 Parts - 2017Silence T-jmNo ratings yet
- Basic Examinations of The Blood: 0.5G SHB/DL of Blood O Hemoglobin Concentration DeterminationDocument14 pagesBasic Examinations of The Blood: 0.5G SHB/DL of Blood O Hemoglobin Concentration DeterminationZllison Mae Teodoro MangabatNo ratings yet
- An Interesting Hematopathology Case: Christopher Julien PGY2Document41 pagesAn Interesting Hematopathology Case: Christopher Julien PGY2Christopher JulienNo ratings yet
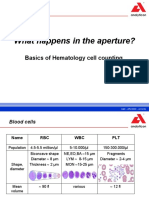
- What Happens in The Aperture?: Basics of Hematology Cell CountingDocument16 pagesWhat Happens in The Aperture?: Basics of Hematology Cell CountingYaser AlaniNo ratings yet
- April RecallsDocument4 pagesApril Recallsfritzie dara f adjilaniNo ratings yet
- Hematology Application For VetDocument56 pagesHematology Application For Vet郑伟健No ratings yet
- Hema LabDocument13 pagesHema LabRothessa CaringalNo ratings yet
- 4-Hematology Analyzer - Detecting Erroneous Blood CountsDocument23 pages4-Hematology Analyzer - Detecting Erroneous Blood CountsRajeshNo ratings yet
- Measurement of Blood Cells and Related ParametersDocument33 pagesMeasurement of Blood Cells and Related ParametersKusuma P SitorusNo ratings yet
- CBC Interpretation GuideDocument45 pagesCBC Interpretation GuideSaifeldein ElimamNo ratings yet
- Hematology Week 1 CBCDocument4 pagesHematology Week 1 CBCMICHELLE RAPELONo ratings yet
- Slide Review CriteriaDocument1 pageSlide Review CriteriaanggaririnNo ratings yet
- XT1800i CustomerDocument74 pagesXT1800i CustomerKesavanVeeraNo ratings yet
- 1.BC 5800 PrincipleDocument37 pages1.BC 5800 PrinciplekiryNo ratings yet
- PBL Hematology 3Document3 pagesPBL Hematology 3Ahmed JabbarNo ratings yet
- Managing Easy Bruising and Fatigue in a Patient with CMLDocument27 pagesManaging Easy Bruising and Fatigue in a Patient with CMLMuhammad BilalNo ratings yet
- 12 CKLDocument7 pages12 CKLAzhar Clinical Laboratory TubeNo ratings yet
- FINAL Automated-HematologyDocument67 pagesFINAL Automated-HematologyDineshprakash GovindhrajNo ratings yet
- Central Philippine University College of Medical Laboratory Science Reticulocyte Count Lab ActivityDocument20 pagesCentral Philippine University College of Medical Laboratory Science Reticulocyte Count Lab ActivityChelsea Padilla Delos ReyesNo ratings yet
- Brochure Balio Ox-560-Ret enDocument2 pagesBrochure Balio Ox-560-Ret enMo AlyNo ratings yet
- Peripheral Blood Smear in Anaemia: Key Findings and Differential DiagnosisDocument77 pagesPeripheral Blood Smear in Anaemia: Key Findings and Differential Diagnosisarthur guytonNo ratings yet
- Laboratory Technology: Flow Cytometry Principles and Application in HematologyDocument40 pagesLaboratory Technology: Flow Cytometry Principles and Application in HematologyYuli RohmaNo ratings yet
- Sine PPT XN Series Utc 15 Sept 2023Document115 pagesSine PPT XN Series Utc 15 Sept 2023sari.b.meilindaNo ratings yet
- CASE STUDY: B-ALL WITH APLASTIC ANEMIADocument15 pagesCASE STUDY: B-ALL WITH APLASTIC ANEMIAShakira HashimNo ratings yet
- Automation in HaematologyDocument67 pagesAutomation in Haematologyk11a1r18No ratings yet
- How To Examine A Blood FilmDocument16 pagesHow To Examine A Blood FilmGretchel PontilarNo ratings yet
- How To Examine A Blood Film: Reem AlsolamiDocument16 pagesHow To Examine A Blood Film: Reem AlsolamiJill ValdesNo ratings yet
- 11 - Hematology Analyzers - Cell CountersDocument19 pages11 - Hematology Analyzers - Cell CountersMohamed YousifNo ratings yet
- Pre Fi HemaDocument7 pagesPre Fi HemaRoyPintorNo ratings yet
- 1.6+7 Laboratory Investigation and Film Interpretation WITHOUT ANSWERSDocument21 pages1.6+7 Laboratory Investigation and Film Interpretation WITHOUT ANSWERSAlex KamougerosNo ratings yet
- By Dr. Richa SharmaDocument51 pagesBy Dr. Richa SharmaTrần Thanh ViệnNo ratings yet
- 【Zybio】Z3 Service Training PPT-Distributor 20200110Document116 pages【Zybio】Z3 Service Training PPT-Distributor 20200110Fermin Tafur Lliuya100% (1)
- Hematology3 10Document23 pagesHematology3 10MohamedKecibaNo ratings yet
- Hematologic ProceduresDocument59 pagesHematologic Proceduresjomel rondinaNo ratings yet
- 1 Cell Counts and Leucocyte Differential CountDocument58 pages1 Cell Counts and Leucocyte Differential CountGloria Grace100% (1)
- Rarwrmicroscopic Examination of Urine: RCF 1.118 X 10 XR CMXRPMDocument13 pagesRarwrmicroscopic Examination of Urine: RCF 1.118 X 10 XR CMXRPMpixiedustNo ratings yet
- Education and Laboratory Testing for COVID-19Document61 pagesEducation and Laboratory Testing for COVID-19mulyadi diningrum100% (1)
- 166 370 1 PBDocument5 pages166 370 1 PBLydya SetyaNo ratings yet
- 05 XE-Series Flagging Guide 12-2008 Complete-20110708-114552Document45 pages05 XE-Series Flagging Guide 12-2008 Complete-20110708-114552kajal4evaNo ratings yet
- Laboratory Management 2Document28 pagesLaboratory Management 2Laboratorium Ansari SalehNo ratings yet
- RSUD Anshari Saleh Banjarmasin Calibration ReportDocument4 pagesRSUD Anshari Saleh Banjarmasin Calibration ReportLaboratorium Ansari SalehNo ratings yet
- Performa Viper20652555 - 2016-09-22 18 - 25Document2 pagesPerforma Viper20652555 - 2016-09-22 18 - 25Laboratorium Ansari SalehNo ratings yet
- Accu-Chek Smart Pix Manual-EN-2.2.1Document190 pagesAccu-Chek Smart Pix Manual-EN-2.2.1Laboratorium Ansari SalehNo ratings yet
- Performa Viper20614935 - 2016-09-22 18 - 30Document8 pagesPerforma Viper20614935 - 2016-09-22 18 - 30Laboratorium Ansari SalehNo ratings yet
- Viral Load CD4 Cells and AntibodiesDocument22 pagesViral Load CD4 Cells and AntibodiesLaboratorium Ansari SalehNo ratings yet
- Performa Viper20652555 - 2016-09-22 13 - 31Document2 pagesPerforma Viper20652555 - 2016-09-22 13 - 31Laboratorium Ansari SalehNo ratings yet
- Sandi Alphabet NasionalDocument2 pagesSandi Alphabet NasionalLaboratorium Ansari SalehNo ratings yet
- Combostik R 300Document1 pageCombostik R 300Laboratorium Ansari SalehNo ratings yet
- Laboratory Management 1Document33 pagesLaboratory Management 1Laboratorium Ansari SalehNo ratings yet
- Immunologi 1Document47 pagesImmunologi 1Laboratorium Ansari SalehNo ratings yet
- Prinsip & Teknologi HA Fix - YuliusDocument26 pagesPrinsip & Teknologi HA Fix - YuliusduckshaNo ratings yet
- Gastroenterohepatology 1Document33 pagesGastroenterohepatology 1Laboratorium Ansari SalehNo ratings yet
- SYMPO 2-2 Continuing Professional Development Program For Clinical Laboratory - Faridah PDFDocument24 pagesSYMPO 2-2 Continuing Professional Development Program For Clinical Laboratory - Faridah PDFLaboratorium Ansari SalehNo ratings yet
- Leukemia Panel Sample Report 2Document2 pagesLeukemia Panel Sample Report 2kurd kar2No ratings yet
- Clinical Manifestations, Pathologic Features, and Diagnosis of Acute Myeloid Leukemia - UpToDateDocument6 pagesClinical Manifestations, Pathologic Features, and Diagnosis of Acute Myeloid Leukemia - UpToDateMariaLuizaAssisNo ratings yet
- G. Mauger - Cours de Langue Et de Civilisation FrançaisesDocument619 pagesG. Mauger - Cours de Langue Et de Civilisation FrançaisesAdrian Mucileanu0% (1)
- Table S1. Examples of Involvement of GSK-3 Isoforms in Cancer. Cancer Type (Alphabetical) GSK-3 Isoform Function Type of Study ReferenceDocument17 pagesTable S1. Examples of Involvement of GSK-3 Isoforms in Cancer. Cancer Type (Alphabetical) GSK-3 Isoform Function Type of Study ReferenceJessica Asitimbay ZuritaNo ratings yet
- Price List Wef 01-Nov2006 NewDocument107 pagesPrice List Wef 01-Nov2006 Newapi-3695832No ratings yet
- Archives of Pathology & Laboratory Medicine Online - Acute Leukemia Immunohistochemistry - A Systematic Diagnostic ApproachDocument13 pagesArchives of Pathology & Laboratory Medicine Online - Acute Leukemia Immunohistochemistry - A Systematic Diagnostic Approachpooo80No ratings yet
- MA251 Computer Assessment: "Survival Analysis" Answer Key: The Saylor Foundation Page 1 of 1Document1 pageMA251 Computer Assessment: "Survival Analysis" Answer Key: The Saylor Foundation Page 1 of 1thermopolis3012No ratings yet
- Acute Erythroid Leukemia: Review ArticleDocument10 pagesAcute Erythroid Leukemia: Review Articlemita potabugaNo ratings yet
- Benzene and Cancer RiskDocument8 pagesBenzene and Cancer Riskايدي قراند 6No ratings yet
- MUST To KNOW in Hematology1-1Document45 pagesMUST To KNOW in Hematology1-1Jez Mendoza ManuelNo ratings yet
- Aspecte Computer Tomografic in Diagnosticul CanceruluiDocument6 pagesAspecte Computer Tomografic in Diagnosticul CanceruluiOana DrăganNo ratings yet
- Leukemia Cutis in Childhood Acute Myeloid.6Document3 pagesLeukemia Cutis in Childhood Acute Myeloid.6fikriafisNo ratings yet
- Hodgkin OEPA-COPDACDocument7 pagesHodgkin OEPA-COPDACJOHN LOPERANo ratings yet
- LeukemiasDocument15 pagesLeukemiasAncy VarkeyNo ratings yet
- Haemato PathofeDocument32 pagesHaemato PathofenorisahnirishNo ratings yet
- An Updated Approach To The Diagnosis of Myeloid Leukemia CutisDocument10 pagesAn Updated Approach To The Diagnosis of Myeloid Leukemia CutisfikriafisNo ratings yet
- Teruko Sakurai Japanese Color Harmony DictionaryDocument22 pagesTeruko Sakurai Japanese Color Harmony DictionaryLily AddamsNo ratings yet
- Khat ThesisDocument4 pagesKhat Thesisbkx8wryp100% (2)
- Adult Health III Final Study GuideDocument12 pagesAdult Health III Final Study GuideRyanne JNo ratings yet
- Tin LeukemiaDocument15 pagesTin LeukemiaKristine YoungNo ratings yet
- INP CU 9 - Bleeding DisorderDocument9 pagesINP CU 9 - Bleeding DisorderMichelle Gliselle Guinto MallareNo ratings yet
- Who 2016Document35 pagesWho 2016Herlina InaNo ratings yet
- Pediatric LeukemiasDocument42 pagesPediatric LeukemiasslyfoxkittyNo ratings yet
- Leukemia Infographic PDFDocument1 pageLeukemia Infographic PDFPriyanka KhuranaNo ratings yet
- Literature Review 1Document3 pagesLiterature Review 1api-534071581No ratings yet