You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Compare Competencies Cross-Match SkillsDocument5 pagesCompare Competencies Cross-Match Skillsmariannepunzalan33% (3)
- 01A SELF-ASSESSMENT CHECK LIST (Done)Document3 pages01A SELF-ASSESSMENT CHECK LIST (Done)mariannepunzalanNo ratings yet
- 01A SELF-ASSESSMENT CHECK LIST (Done)Document3 pages01A SELF-ASSESSMENT CHECK LIST (Done)mariannepunzalanNo ratings yet
- 01A SELF-ASSESSMENT CHECK LIST (Done)Document3 pages01A SELF-ASSESSMENT CHECK LIST (Done)mariannepunzalanNo ratings yet
- Trainee'S Record BookDocument10 pagesTrainee'S Record BookmariannepunzalanNo ratings yet
- 07 Training Program EvaluationDocument5 pages07 Training Program EvaluationmariannepunzalanNo ratings yet
- 07 Training Program EvaluationDocument5 pages07 Training Program EvaluationmariannepunzalanNo ratings yet
- Trainee'S Record Book: Cadlan, Pili, Camarines SurDocument12 pagesTrainee'S Record Book: Cadlan, Pili, Camarines SurmariannepunzalanNo ratings yet
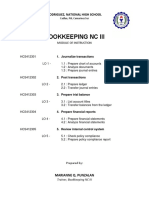
- Bookkeeping NC Iii: Rodriguez, National High SchoolDocument1 pageBookkeeping NC Iii: Rodriguez, National High SchoolmariannepunzalanNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Syllabus DiplomaDocument4 pagesSyllabus Diplomashahbaz alamNo ratings yet
- Effect of Container Size on Candle BurningDocument4 pagesEffect of Container Size on Candle BurningAinul Zarina AzizNo ratings yet
- Bharath Kumar: Software Development Engineer IDocument3 pagesBharath Kumar: Software Development Engineer IAlton AbrahamNo ratings yet
- Boy Scouts Crew MembershipDocument23 pagesBoy Scouts Crew MembershipAldrin M. Obias100% (1)
- APC Boosts Polypropylene OperationDocument6 pagesAPC Boosts Polypropylene OperationJuan AlejandroNo ratings yet
- Junior HSE AssistantDocument2 pagesJunior HSE AssistantMuhammad AdnanNo ratings yet
- Emirates Future International Academy Grade-5 WorksheetDocument2 pagesEmirates Future International Academy Grade-5 WorksheetSajir ThiyamNo ratings yet
- MCHS 1965 YearbookDocument112 pagesMCHS 1965 YearbookMater Dei Catholic High SchoolNo ratings yet
- Hand Book of Information New 2018 19 Final 9mayDocument247 pagesHand Book of Information New 2018 19 Final 9mayGagan BhatiaNo ratings yet
- Pancasila Character EducationDocument6 pagesPancasila Character EducationDaniel Prayoga D100% (1)
- Camp Greene: A Summer Day Camp Program GuideDocument32 pagesCamp Greene: A Summer Day Camp Program Guideapi-551810918No ratings yet
- Adult Learning An OverviewDocument11 pagesAdult Learning An OverviewKhalif AziziNo ratings yet
- Music and Translation: Palgrave Studies IN Translating AND InterpretingDocument417 pagesMusic and Translation: Palgrave Studies IN Translating AND InterpretingBen Nyaman0% (1)
- Mapeh 10 Curriculum MapDocument9 pagesMapeh 10 Curriculum MapJoshua LamzonNo ratings yet
- OlanipekunDocument3 pagesOlanipekunAnesu MasirahaNo ratings yet
- Minit Mesyuarat Kokurikulum KALI Ke-2 - 2020Document6 pagesMinit Mesyuarat Kokurikulum KALI Ke-2 - 2020ruzilawatiNo ratings yet
- Police Miscue Told in Bus Incident: Case StudyDocument19 pagesPolice Miscue Told in Bus Incident: Case StudyAtul SharmaNo ratings yet
- Final Dissertation Paper - Role of Open Spaces in LearningDocument8 pagesFinal Dissertation Paper - Role of Open Spaces in LearninghasnaNo ratings yet
- Lesson Plan ReadingDocument4 pagesLesson Plan ReadingnelieltuodeshvankNo ratings yet
- TERNA ENGINEERING COLLEGE ACADEMIC CALENDARDocument5 pagesTERNA ENGINEERING COLLEGE ACADEMIC CALENDARPuppysinghNo ratings yet
- Chenrezig MeditationDocument2 pagesChenrezig MeditationMonge DorjNo ratings yet
- Chem 105 Syllabus 2013 SpringDocument4 pagesChem 105 Syllabus 2013 SpringemuphychemNo ratings yet
- A Practical Guide To Behavioral Research Tools and Techniques - Capítulo 01 PDFDocument9 pagesA Practical Guide To Behavioral Research Tools and Techniques - Capítulo 01 PDFdani_g_1987No ratings yet
- eYRC-2016: Track 1 No Objection Certificate (NOC) FormatDocument2 pageseYRC-2016: Track 1 No Objection Certificate (NOC) FormatManthanNo ratings yet
- GE 8 EthcsDocument22 pagesGE 8 EthcsWilliam Soneja CalapiniNo ratings yet
- 1.4 Components of Ethology: InstinctDocument7 pages1.4 Components of Ethology: InstinctAndreea BradNo ratings yet
- Duolingo Homework PDF 22 MayDocument6 pagesDuolingo Homework PDF 22 MayPriya PriyaNo ratings yet
- Bansal Institute of Engineering & Technology, LucknowDocument22 pagesBansal Institute of Engineering & Technology, Lucknowshivansh sahu100No ratings yet
- Marketing Launchpad Screening Test PrepDocument10 pagesMarketing Launchpad Screening Test PrepsuryaNo ratings yet
- Lesson Plan Adjectives Comparative and SuperlativeDocument12 pagesLesson Plan Adjectives Comparative and SuperlativeZeliha TileklioğluNo ratings yet