You might also like
- Wrist or Hand Disability IndexDocument1 pageWrist or Hand Disability Indexdwi danangNo ratings yet
- Neck Disability IndexDocument2 pagesNeck Disability IndexCloudy ValenNo ratings yet
- Wrist Hand Functional AssessmentDocument1 pageWrist Hand Functional AssessmentPriska ChrisandyNo ratings yet
- Wrist Joint Anatomy and TestsDocument38 pagesWrist Joint Anatomy and Testscamy bhagatNo ratings yet
- TMD Disability IndexDocument2 pagesTMD Disability IndexSamuel Nanda LazuardiNo ratings yet
- Development of The Early Activity Scale For EnduranceDocument1 pageDevelopment of The Early Activity Scale For EnduranceAsesino GuerreroNo ratings yet
- Neck Disability IndexDocument1 pageNeck Disability IndexmanusiddNo ratings yet
- Algoritma LeDocument1 pageAlgoritma LerimaNo ratings yet
- Pediatric Balance Scale Sixteen Balance TestDocument8 pagesPediatric Balance Scale Sixteen Balance TestEddy Lanang'e JagadNo ratings yet
- Microwave Diathermy 2013Document27 pagesMicrowave Diathermy 2013Faisal QureshiNo ratings yet
- Special Tests For WristDocument13 pagesSpecial Tests For WristSaif Ahmed LariNo ratings yet
- Chest Physio RCT Finds No Benefit in Pediatric PneumoniaDocument7 pagesChest Physio RCT Finds No Benefit in Pediatric Pneumoniaaufa memeyNo ratings yet
- Arthrogryposis Congenital ContractureDocument32 pagesArthrogryposis Congenital ContractureMayesa Akiro100% (1)
- Jurnal Tennis ElbowDocument5 pagesJurnal Tennis ElbowMuhamad Fahrizal RilahiNo ratings yet
- Nyeri Pada Tennis Elbow Tipe IIDocument14 pagesNyeri Pada Tennis Elbow Tipe IIlisaNo ratings yet
- William Vs MC Kenzie-1Document4 pagesWilliam Vs MC Kenzie-1DefaNo ratings yet
- Drop Foot Therapy PracticesDocument3 pagesDrop Foot Therapy PracticesRiina HapsariiNo ratings yet
- Loss of Sensation in the Medial PalmDocument8 pagesLoss of Sensation in the Medial Palmananya mishraNo ratings yet
- Normal Human LocomotionDocument16 pagesNormal Human LocomotionWendy NgNo ratings yet
- Awareness of Text Neck Syndrome in Young-Adult Pop PDFDocument5 pagesAwareness of Text Neck Syndrome in Young-Adult Pop PDFBarkha FulwaniNo ratings yet
- Journal of Hand Therapy: Hayat Hamzeh PT, MSC, Mohammad Madi PT, PHD, Alia A. Alghwiri PT, PHD, Ziad Hawamdeh MD, PHDDocument9 pagesJournal of Hand Therapy: Hayat Hamzeh PT, MSC, Mohammad Madi PT, PHD, Alia A. Alghwiri PT, PHD, Ziad Hawamdeh MD, PHDWinda FRNo ratings yet
- Fugl-Meyer Assessment Lower Extremity (Fma-Le) Assessment of Sensorimotor FunctionDocument2 pagesFugl-Meyer Assessment Lower Extremity (Fma-Le) Assessment of Sensorimotor FunctionDũng HoàngNo ratings yet
- Shortwave and Microwave Diathermy Techniques and ApplicationsDocument17 pagesShortwave and Microwave Diathermy Techniques and ApplicationsRidwan Hadinata SalimNo ratings yet
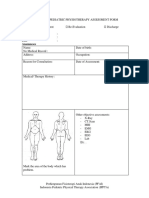
- Form PEMERIKSANAAN UMUM FT ANAK 300419Document4 pagesForm PEMERIKSANAAN UMUM FT ANAK 300419vanoNo ratings yet
- Rehabilitation of Cerebral Palsy & Motor DelayDocument49 pagesRehabilitation of Cerebral Palsy & Motor DelayasloocltNo ratings yet
- Sensory ExamDocument2 pagesSensory ExamShannen Christelle AndradeNo ratings yet
- Capsular pattern identification in idiopathic frozen shoulderDocument11 pagesCapsular pattern identification in idiopathic frozen shoulderRhany JulyatiNo ratings yet
- Jurnal Ilmiah Fisioterapi (JIF) Volume 03 Nomor 01 Februari 2020Document6 pagesJurnal Ilmiah Fisioterapi (JIF) Volume 03 Nomor 01 Februari 2020Putri teopani saragihNo ratings yet
- Matsyasana (Fish Pose) : TechniqueDocument1 pageMatsyasana (Fish Pose) : TechniqueKarisma SenapatiNo ratings yet
- Shoulder Pain Index for Assessing DisabilityDocument2 pagesShoulder Pain Index for Assessing DisabilityLindaPramusintaNo ratings yet
- Pelvic Floor Impact Questionnaire (PFIQ-7)Document2 pagesPelvic Floor Impact Questionnaire (PFIQ-7)Dharitri PurohitNo ratings yet
- Shoulder Pain and Disability Index SPADI .44Document1 pageShoulder Pain and Disability Index SPADI .44knikmahNo ratings yet
- Week 1 and 2 PCP Workbook QuestionsDocument4 pagesWeek 1 and 2 PCP Workbook Questionsapi-479717740100% (1)
- Romberg Test Examines Proprioception DeficitDocument7 pagesRomberg Test Examines Proprioception DeficitDwi P Ramadhani0% (1)
- 4 Brunnstrom ApproachDocument18 pages4 Brunnstrom ApproachHabibieNaufal ChannelNo ratings yet
- Efektivitas Peningkatan Aktifitas Fungsional Dengan Intervensi Ice Massage Dan Terapi Latihan Pada Kasus Plantar FasciitisDocument8 pagesEfektivitas Peningkatan Aktifitas Fungsional Dengan Intervensi Ice Massage Dan Terapi Latihan Pada Kasus Plantar FasciitisTiara PutriNo ratings yet
- Hip Replacement GuideDocument28 pagesHip Replacement GuideZulaika NaisNo ratings yet
- Contrast Bath - MKKDocument10 pagesContrast Bath - MKKKishore KumarNo ratings yet
- BFO-Ankle Foot Orthotics - Introduction and Biomechanical PrinciplesDocument9 pagesBFO-Ankle Foot Orthotics - Introduction and Biomechanical PrinciplesnovitaNo ratings yet
- Rom PDFDocument6 pagesRom PDFPrivat EtavirpNo ratings yet
- PIT XIX PERDOSRI Virtual 2020 004Document3 pagesPIT XIX PERDOSRI Virtual 2020 004Dinda SurantoNo ratings yet
- Twstrs ScalaDocument2 pagesTwstrs ScalaAlin Lin-LinNo ratings yet
- Skin Mechanical Properties - ArinSDocument26 pagesSkin Mechanical Properties - ArinSJack Flow ClickNo ratings yet
- Lund and Browder ChartDocument1 pageLund and Browder ChartFirras SalsabilaNo ratings yet
- Tumbang ICF ADHDDocument1 pageTumbang ICF ADHDNovita OktavianaNo ratings yet
- De Quervain SyndromeDocument5 pagesDe Quervain SyndromePaula ZorziNo ratings yet
- Understanding the Underlying Process of Trauma and Its TreatmentDocument3 pagesUnderstanding the Underlying Process of Trauma and Its TreatmentannyNo ratings yet
- MMT (Manual Muscle Testing)Document18 pagesMMT (Manual Muscle Testing)Estu MahendraNo ratings yet
- Functional Reach Arm Test (FRT)Document7 pagesFunctional Reach Arm Test (FRT)AnisDwiUlfahndariNo ratings yet
- Low Back Pain Lapkas 2Document27 pagesLow Back Pain Lapkas 2rini najoanNo ratings yet
- Claw HandDocument16 pagesClaw HandArum MaharaniNo ratings yet
- Patologi KardiopulmonalDocument43 pagesPatologi Kardiopulmonal9661jackNo ratings yet
- Beighton Hypermobility ScoreDocument2 pagesBeighton Hypermobility ScoreVishal RautNo ratings yet
- Calcaneus SpurDocument21 pagesCalcaneus SpurekoNo ratings yet
- Short Wave Diathermy Is Defined As The Clinical Application of High Frequency Alternating Current, at A Frequency of 27.12Mhz and Wavelength of 11.06 MeterDocument1 pageShort Wave Diathermy Is Defined As The Clinical Application of High Frequency Alternating Current, at A Frequency of 27.12Mhz and Wavelength of 11.06 MeterMohd AsadNo ratings yet
- Harris Hip Score SheetDocument1 pageHarris Hip Score Sheetstevebravo81100% (1)
- Wrist/Hand Disability Index: I Pain Intensity Vi WorkDocument1 pageWrist/Hand Disability Index: I Pain Intensity Vi WorkHumza HamidNo ratings yet
- Wrist or Hand Disability IndexDocument1 pageWrist or Hand Disability IndexHumza HamidNo ratings yet
- InglesDocument46 pagesInglesAzulit KryNo ratings yet
- Oswestry Disability IndexDocument4 pagesOswestry Disability Indexpaulina_810No ratings yet
- Revised MPT OrdinanceDocument90 pagesRevised MPT OrdinancesmrutiptNo ratings yet
- Geriatric Rehab Device Choices: Cane, Crutches, Walker or Forearm Supports for 78yo F after Knee ReplacementDocument31 pagesGeriatric Rehab Device Choices: Cane, Crutches, Walker or Forearm Supports for 78yo F after Knee ReplacementsmrutiptNo ratings yet
- Bachelor of Physiotherapy - BPT: (4 Year Degree Course)Document107 pagesBachelor of Physiotherapy - BPT: (4 Year Degree Course)Ritesh TrivediNo ratings yet
- Basic MPTDocument40 pagesBasic MPTsmrutiptNo ratings yet
- Visual Gait Analysis and Assessment TechniquesDocument22 pagesVisual Gait Analysis and Assessment TechniquesKumar RanjanNo ratings yet
- Understanding Arthrogyposis Multiplex Congenita and Muscular DystrophiesDocument38 pagesUnderstanding Arthrogyposis Multiplex Congenita and Muscular DystrophiessmrutiptNo ratings yet
- Orthopedic Appliances: Inlays Shoes OrthosesDocument20 pagesOrthopedic Appliances: Inlays Shoes OrthosessmrutiptNo ratings yet
- ProsthesisDocument42 pagesProsthesissmrutiptNo ratings yet
- Cerebral PalsyDocument49 pagesCerebral PalsysmrutiptNo ratings yet
- Sports InjuriesDocument29 pagesSports InjuriessmrutiptNo ratings yet
- Local Complication of Local AnesthesiaDocument22 pagesLocal Complication of Local AnesthesiacobacobatestNo ratings yet
- Office OrthopaedicsDocument308 pagesOffice OrthopaedicsJohn Reynolds100% (10)
- Skenario 1 Kelompok 8Document16 pagesSkenario 1 Kelompok 8araahNo ratings yet
- Lymphomyosot Aids Conventional Therapy in Diabetic Peripherial Neuropathy 2003Document8 pagesLymphomyosot Aids Conventional Therapy in Diabetic Peripherial Neuropathy 2003Dr. Nancy MalikNo ratings yet
- Kiyoshige Ohseto, Hiroyuki Uchino, Hiroki Iida - Nerve Blockade and Interventional Therapy (2019, Springer Japan)Document344 pagesKiyoshige Ohseto, Hiroyuki Uchino, Hiroki Iida - Nerve Blockade and Interventional Therapy (2019, Springer Japan)Xunyao LuNo ratings yet
- Pri̇locai̇ne HCL MSDSDocument10 pagesPri̇locai̇ne HCL MSDSEsin KahramanNo ratings yet
- Food Safety and HygieneDocument10 pagesFood Safety and HygieneBright KapapaNo ratings yet
- Assessment of Skin Functions and StructuresDocument65 pagesAssessment of Skin Functions and StructuresVinzii Drt100% (1)
- CAGE Test Alcool, CAGE Test Droguri, Test AUDIT Pentru Alcoolism. Ce Este Adictia. Coping Si TratamentDocument35 pagesCAGE Test Alcool, CAGE Test Droguri, Test AUDIT Pentru Alcoolism. Ce Este Adictia. Coping Si TratamentAnonymous KgUtPlkjNo ratings yet
- Biomechanical PrinciplesDocument84 pagesBiomechanical PrinciplesbhongskirnNo ratings yet
- Peripheral Neuropathies PathoDocument2 pagesPeripheral Neuropathies PathoSOLEIL LOUISE LACSON MARBASNo ratings yet
- 09 Lec NotesDocument9 pages09 Lec NotesEvilasio CostaNo ratings yet
- 5 177096869007065747 PDFDocument59 pages5 177096869007065747 PDFsillypolo100% (2)
- 1631 DN4 QuestionnaireDocument2 pages1631 DN4 QuestionnaireRaywa 217100% (1)
- Guillain-Barré Syndrome: Causes, Symptoms, TreatmentDocument26 pagesGuillain-Barré Syndrome: Causes, Symptoms, TreatmentArslan AslamNo ratings yet
- Abies Can-Antimonio TDocument180 pagesAbies Can-Antimonio TArellano M VictorNo ratings yet
- LPUN College of Nursing Guide for Nursing ProcessDocument6 pagesLPUN College of Nursing Guide for Nursing ProcessCaryl EteNo ratings yet
- Goodman & Snyder: Differential Diagnosis For Physical Therapists, 5th EditionDocument4 pagesGoodman & Snyder: Differential Diagnosis For Physical Therapists, 5th EditionCyndi MenesesNo ratings yet
- Understanding Cancer Pain 2021Document68 pagesUnderstanding Cancer Pain 2021AnestilNo ratings yet
- Diadynamic Currents The Purpose of The Class: To Study The Biophysical Basis of AC Action PhysicalDocument5 pagesDiadynamic Currents The Purpose of The Class: To Study The Biophysical Basis of AC Action PhysicalKumar AdityaNo ratings yet
- Pressure Pointer ManualDocument17 pagesPressure Pointer ManualsorinmoroNo ratings yet
- Terms and Strategies For Medical RecordsDocument13 pagesTerms and Strategies For Medical RecordsJohn Balas AjenasNo ratings yet
- Peripheral Nerve Diseases The BARE ESSENTIALSDocument10 pagesPeripheral Nerve Diseases The BARE ESSENTIALSGustiAyuCyntia100% (1)
- Nerve Damage of Diabetes ExplainedDocument12 pagesNerve Damage of Diabetes ExplainedtaqiedaNo ratings yet
- Recall 139, Sum 2.3.13 AMC CLINICALDocument34 pagesRecall 139, Sum 2.3.13 AMC CLINICALAMMARA100% (3)
- Orthopedic NursingDocument9 pagesOrthopedic Nursingsilimaanghang100% (2)
- Neurovascular Assessment: Detecting Early Signs of CompromiseDocument4 pagesNeurovascular Assessment: Detecting Early Signs of CompromiseNatalia OrtizNo ratings yet
- Office ErgonomicsDocument28 pagesOffice ErgonomicsAnonymous iI88Lt100% (2)
- Local Complications of LaDocument29 pagesLocal Complications of LaaakiNo ratings yet
- America Materia Medica PDFDocument470 pagesAmerica Materia Medica PDFSudhakarNo ratings yet