You might also like
- 10 1016@j Hoc 2019 03 006-2Document12 pages10 1016@j Hoc 2019 03 006-2Bruna AngeloNo ratings yet
- Emerging Treatments For Crohn's Disease: Cells, Surgery, and Novel TherapeuticsDocument10 pagesEmerging Treatments For Crohn's Disease: Cells, Surgery, and Novel Therapeuticsellya theresiaNo ratings yet
- 1 s2.0 S0923753419321301 MainDocument4 pages1 s2.0 S0923753419321301 MainVilanNo ratings yet
- Acute Myeloid Leukemia...Document20 pagesAcute Myeloid Leukemia...hemendre0% (1)
- New Drugs and Pharmacological Interactions in Real LifeDocument5 pagesNew Drugs and Pharmacological Interactions in Real LifecarolinaNo ratings yet
- British Medical Bulletin Advance Access published November 22, 2012Document22 pagesBritish Medical Bulletin Advance Access published November 22, 2012eva yustianaNo ratings yet
- Van Erp Et Al, 2009, Clinical Pharmacokinetics of Tyrosine Kinase InhibitorsDocument15 pagesVan Erp Et Al, 2009, Clinical Pharmacokinetics of Tyrosine Kinase Inhibitorsdhania novitasariNo ratings yet
- Jurnal Limfoma Sel BDocument12 pagesJurnal Limfoma Sel BDian Pratiwi PutriNo ratings yet
- Cancers: Advances in Acute Myeloid Leukemia: Recently Approved Therapies and Drugs in DevelopmentDocument32 pagesCancers: Advances in Acute Myeloid Leukemia: Recently Approved Therapies and Drugs in DevelopmentDanyal SiddiquiNo ratings yet
- 10 1016@j Ucl 2020 07 009Document13 pages10 1016@j Ucl 2020 07 009Posgrado CirugiaNo ratings yet
- Pembrolizumab in MSI-H DMMR Advanced Colorectal Cancer A New Standard of CareDocument3 pagesPembrolizumab in MSI-H DMMR Advanced Colorectal Cancer A New Standard of CareasdffdsaNo ratings yet
- J J Rad Oncol 3 2 029-2Document4 pagesJ J Rad Oncol 3 2 029-2Angela PagliusoNo ratings yet
- Pembrolizumab For Advanced Cervical Cancer Safety and EfficacyDocument9 pagesPembrolizumab For Advanced Cervical Cancer Safety and EfficacyluizaNo ratings yet
- New JaneDocument34 pagesNew JaneniputusellyowNo ratings yet
- Radioimmunotherapy With Tositumomab and Iodine-131 Tositumomab For Non-Hodgkin's LymphomaDocument8 pagesRadioimmunotherapy With Tositumomab and Iodine-131 Tositumomab For Non-Hodgkin's LymphomaVera MirandaNo ratings yet
- Fonc 09 00396Document8 pagesFonc 09 00396asdffdsaNo ratings yet
- A Combined Preclinical Therapy of Cannabinoids and Temozolomide Against Glioma - FullDocument14 pagesA Combined Preclinical Therapy of Cannabinoids and Temozolomide Against Glioma - FullacbgdvNo ratings yet
- Novel Immunotherapeutics in B-Cell Precursor ALLDocument23 pagesNovel Immunotherapeutics in B-Cell Precursor ALLqcywh2000No ratings yet
- Emerging Epigenetic-Modulating - Sermer2019Document14 pagesEmerging Epigenetic-Modulating - Sermer2019Diego AntunezNo ratings yet
- Researcharticle Open AccessDocument13 pagesResearcharticle Open AccessManuela Martín-Bejarano GarcíaNo ratings yet
- Multiple Myeloma - A Quick Reflection On The Fast Progress 2013Document326 pagesMultiple Myeloma - A Quick Reflection On The Fast Progress 2013Daoud IssaNo ratings yet
- Cancers 15 03408 v2Document14 pagesCancers 15 03408 v2Jesus Barraza SánchezNo ratings yet
- Drug-Induced PD-L1 Expression and Cell Stress Response in Breast Cancer Cells Can Be Balanced by Drug CombinationDocument8 pagesDrug-Induced PD-L1 Expression and Cell Stress Response in Breast Cancer Cells Can Be Balanced by Drug Combinationygilad9139No ratings yet
- Lancet 2021 Immune Checkpoint Inhibitor Petit ArticleDocument2 pagesLancet 2021 Immune Checkpoint Inhibitor Petit ArticleJeanne LahogueNo ratings yet
- Cells: Highlights in Resistance Mechanism Pathways For Combination TherapyDocument29 pagesCells: Highlights in Resistance Mechanism Pathways For Combination TherapyHeru SigitNo ratings yet
- 2018 PharmacogeneticspaperDocument17 pages2018 PharmacogeneticspaperKatzumi MartinezNo ratings yet
- Novos Tratamentos NefritelupicaDocument23 pagesNovos Tratamentos NefritelupicaMaria Eduarda CardosoNo ratings yet
- Chemotherapy-And Cancer-Related Nausea and Vomiting: Table IDocument12 pagesChemotherapy-And Cancer-Related Nausea and Vomiting: Table IVayu PuthraNo ratings yet
- Cannabis Et CancerDocument5 pagesCannabis Et CancerJoaquim MurtinhoNo ratings yet
- Lenalidomide Plus Prednisone Results in Durable Clinical, Histopathologic, and Molecular Responses in Patients With MyelofibrosisDocument7 pagesLenalidomide Plus Prednisone Results in Durable Clinical, Histopathologic, and Molecular Responses in Patients With MyelofibrosisRima RahmounNo ratings yet
- Brown 2014Document9 pagesBrown 2014Rafaela Queiroz MascarenhasNo ratings yet
- New Drugs and Treatment Targets in Psoriasis: Review ArticleDocument7 pagesNew Drugs and Treatment Targets in Psoriasis: Review Article5netNo ratings yet
- Avances en MelanomaDocument11 pagesAvances en MelanomaEdilma VargasNo ratings yet
- 3 The Emerging Role of Epigenetic Therapeutics in ImmunooncologyDocument38 pages3 The Emerging Role of Epigenetic Therapeutics in ImmunooncologylauraNo ratings yet
- Reardon 2017Document15 pagesReardon 2017Carlos ImasNo ratings yet
- How To Practice Environmental Medicine: The Path AheadDocument8 pagesHow To Practice Environmental Medicine: The Path AheadFabian VolpeNo ratings yet
- Cheah 2015Document8 pagesCheah 2015Bruna AngeloNo ratings yet
- Jop 18 00005Document4 pagesJop 18 00005Anonymous 8KN8IR1GTWNo ratings yet
- Emerging Therapies in Chronic Lymphocytic Leukemia: Reslan Lina and Dumontet CharlesDocument17 pagesEmerging Therapies in Chronic Lymphocytic Leukemia: Reslan Lina and Dumontet Charleskj185No ratings yet
- Jurnal AntibodimonoklonalDocument11 pagesJurnal AntibodimonoklonalKartika PuspitaningrumNo ratings yet
- Maly 2016Document9 pagesMaly 2016Jose Angel AbadíaNo ratings yet
- PHD Thesis in Pancreatic CancerDocument7 pagesPHD Thesis in Pancreatic Cancerzxtccvgld100% (2)
- Adaptation TTT Dans LHDocument16 pagesAdaptation TTT Dans LHmohamed maaloulNo ratings yet
- Bencimidazoles Anti CáncerDocument10 pagesBencimidazoles Anti CáncerEylan Goitia De GonzálezNo ratings yet
- A Comprehensive Review of Current Treatments For Granulomatous Cheilitis (British Journal of Dermatology, Vol. 166, Issue 5) (2012)Document4 pagesA Comprehensive Review of Current Treatments For Granulomatous Cheilitis (British Journal of Dermatology, Vol. 166, Issue 5) (2012)Padmapriya SrinivasanNo ratings yet
- 2008 - Antituberculosis Drug-Induced Hepatotoxicity Concise Up-To-Date ReviewDocument12 pages2008 - Antituberculosis Drug-Induced Hepatotoxicity Concise Up-To-Date ReviewCarlos LuqueNo ratings yet
- Atezolizumab and Nab-Paclitaxel in Advanced Triple-Negative Breast CancerDocument14 pagesAtezolizumab and Nab-Paclitaxel in Advanced Triple-Negative Breast CancerRodrigoSachiFreitasNo ratings yet
- Defining The Stages of Aggressive Non-Hodgkin's LymphomaDocument3 pagesDefining The Stages of Aggressive Non-Hodgkin's LymphomaomarbenhagiNo ratings yet
- Combinatorial Drug Therapy For Cancer in The Post-Genomic EraDocument13 pagesCombinatorial Drug Therapy For Cancer in The Post-Genomic EraBobNo ratings yet
- Pharmacotherapy of Cancer Cell Cycle and Anti-Cancer DrugsDocument14 pagesPharmacotherapy of Cancer Cell Cycle and Anti-Cancer DrugsElodie NguetieNo ratings yet
- Polymer Drug Conjugates As Potent Against Cellular ApoptosisDocument8 pagesPolymer Drug Conjugates As Potent Against Cellular ApoptosisGourav DasNo ratings yet
- New Drugs ArtritisDocument13 pagesNew Drugs ArtritisqfecrespoNo ratings yet
- Curr Med Chem 16182235-22602009Document26 pagesCurr Med Chem 16182235-22602009ZozoNo ratings yet
- Avelumab 45Document10 pagesAvelumab 45bawoji1763No ratings yet
- Rheumatology 05Document6 pagesRheumatology 05C Bala DiwakeshNo ratings yet
- Mondello Et Al. - 2016 - 90 Y-Ibritumomab Tiuxetan A Nearly Forgotten OpportunityDocument13 pagesMondello Et Al. - 2016 - 90 Y-Ibritumomab Tiuxetan A Nearly Forgotten OpportunityacbgdvNo ratings yet
- Acute Myeloid Leukemia: Current Progress and Future DirectionsDocument25 pagesAcute Myeloid Leukemia: Current Progress and Future DirectionsDiahNo ratings yet
- TTT of CancerDocument10 pagesTTT of Cancerali ahmedNo ratings yet
- Ijms 24 02542Document3 pagesIjms 24 02542Frank MacíasNo ratings yet
- Lung Isolation Techniques - UpToDateDocument9 pagesLung Isolation Techniques - UpToDateAna Belén Artero CastañoNo ratings yet
- Guidelines For Phase I Clinical Trials 2018 Edition 20180626Document72 pagesGuidelines For Phase I Clinical Trials 2018 Edition 20180626Juan Vasquez100% (1)
- The Treatment For Dengue Fever Is Often Supportive in NatureDocument8 pagesThe Treatment For Dengue Fever Is Often Supportive in NatureJames FabioNo ratings yet
- OET Reading 15Document15 pagesOET Reading 15lira may azarceNo ratings yet
- PNF Manual For Primary Healthcare PDFDocument317 pagesPNF Manual For Primary Healthcare PDFtej0331No ratings yet
- Lplpo UnitDocument31 pagesLplpo UnitAnis mudawamahNo ratings yet
- ET TubeDocument4 pagesET TuberumasadraunaNo ratings yet
- Pharmacy Directory CADocument45 pagesPharmacy Directory CAprogomezkylieNo ratings yet
- Implant Catalogue: Your Local Mentor DistributorDocument36 pagesImplant Catalogue: Your Local Mentor DistributorSofia VasconcellosNo ratings yet
- Essential Drug List: (Accessed 24 April 2007)Document47 pagesEssential Drug List: (Accessed 24 April 2007)Ryan Noel Perez de TagleNo ratings yet
- Mindmap CH 5 Therapeutic ApproachesDocument1 pageMindmap CH 5 Therapeutic ApproachesKshitij DasariNo ratings yet
- Assignments of PGDPSM: An OverviewDocument8 pagesAssignments of PGDPSM: An OverviewPratik YaulNo ratings yet
- Analgesiainratsandmice2 11Document2 pagesAnalgesiainratsandmice2 11Ciong TanNo ratings yet
- Pharmacology Unit 2Document19 pagesPharmacology Unit 2Bea Bianca CruzNo ratings yet
- DRUG STUDY RabiesDocument1 pageDRUG STUDY RabiesFranz RolfNo ratings yet
- AnalisisstockDocument486 pagesAnalisisstockFilipusHendriSuryawanNo ratings yet
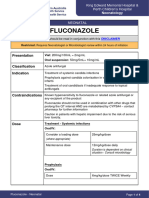
- FluconazoleDocument4 pagesFluconazoleeucaNo ratings yet
- MetoclopramideDocument1 pageMetoclopramideYanejoulce SacanleNo ratings yet
- One PotDocument12 pagesOne PotOgnjenNo ratings yet
- Pharmacology II OutlineDocument52 pagesPharmacology II Outlinerjones53No ratings yet
- FRUSEMIDEDocument3 pagesFRUSEMIDEkrishna chandrakani100% (1)
- Cology Q&A All UnitsDocument51 pagesCology Q&A All UnitsRafiya CNo ratings yet
- Elmiron - E Janssen Nov 2011 Sodium Pentosan PolysulfateDocument18 pagesElmiron - E Janssen Nov 2011 Sodium Pentosan PolysulfateManjit WadhwaNo ratings yet
- Opiate Induced Nausea and Vomiting What Is The.15Document2 pagesOpiate Induced Nausea and Vomiting What Is The.15Riski YustitiaNo ratings yet
- Pharmac KineticsDocument30 pagesPharmac Kineticsimaslov16No ratings yet
- Inventory ManagementDocument24 pagesInventory ManagementMohamed LaghyatiNo ratings yet
- Data Obat Apotek Okt2023Document26 pagesData Obat Apotek Okt2023apoteknyarosiNo ratings yet
- Micardis PlusDocument2 pagesMicardis PlusKristine YoungNo ratings yet
- Phenytoin Sodium 50 MG Film-Coated Tablets (Phenytoin Sodium) PL 16363/0253Document17 pagesPhenytoin Sodium 50 MG Film-Coated Tablets (Phenytoin Sodium) PL 16363/0253Mohammed shamiul ShahidNo ratings yet
- Data Harga Beli BarangDocument78 pagesData Harga Beli BarangAbadiFikarNo ratings yet