You might also like
- DSM 5 OverviewDocument78 pagesDSM 5 Overviewoyehello23No ratings yet
- DSM 5 DiagnosingDocument107 pagesDSM 5 DiagnosingMichel Haddad100% (1)
- A Survival Guide to Understanding the DSM-5Document73 pagesA Survival Guide to Understanding the DSM-5Luke Bacon100% (2)
- The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5)Document42 pagesThe Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5)Mihaela Onisia UngureanuNo ratings yet
- Chapter 3 Notes Abnormal PsychDocument14 pagesChapter 3 Notes Abnormal PsychAnonymous Sfcml4GvZ0% (1)
- Classification Psychiatric DisordersDocument40 pagesClassification Psychiatric DisordersAdrishyaNo ratings yet
- Abnormal Psychology Notes IB SLDocument41 pagesAbnormal Psychology Notes IB SLHilda Hiong100% (4)
- Malingering - Concept and ControversiesDocument40 pagesMalingering - Concept and Controversiesfareed oomer100% (1)
- Differential DiagnosisDocument28 pagesDifferential DiagnosisDr. Khawer BaigNo ratings yet
- A2 Clinical Psychology Revision Notes EdexcelDocument12 pagesA2 Clinical Psychology Revision Notes Edexcelmoniquelouise95100% (1)
- Diagnosis and Treatment of Mental Disorders: An IntroductionFrom EverandDiagnosis and Treatment of Mental Disorders: An IntroductionNo ratings yet
- Inguinal Hernia: Peritoneum, Resulting in A BulgeDocument5 pagesInguinal Hernia: Peritoneum, Resulting in A BulgeJunathan L. Delgado100% (1)
- Clinical & Counseling AssessmentDocument52 pagesClinical & Counseling AssessmentMaica GuceNo ratings yet
- Consultation Liaison PsychiatryDocument57 pagesConsultation Liaison PsychiatryPriyash Jain100% (2)
- 01 Psychiatric Assessment & DSM-5 BBDocument62 pages01 Psychiatric Assessment & DSM-5 BBDhillonvNo ratings yet
- Abnormal Psychology - Past and PresentDocument19 pagesAbnormal Psychology - Past and PresentRizwana MBTNo ratings yet
- DermatologyDocument121 pagesDermatologyjimisurgon83100% (4)
- Overview of The DSM 5Document68 pagesOverview of The DSM 5khalpopoNo ratings yet
- APA DSM 5 Somatic Symptom DisorderDocument2 pagesAPA DSM 5 Somatic Symptom DisordermargauxNo ratings yet
- Dysphagia AssessmentDocument6 pagesDysphagia AssessmentShruti PatilNo ratings yet
- Abnormal Psychology Module 1 Understanding Abnormal BehaviorDocument31 pagesAbnormal Psychology Module 1 Understanding Abnormal BehaviorSumriddhi Srivastava100% (1)
- ThalassemiaDocument16 pagesThalassemiaAry AffandiNo ratings yet
- Se 04 Abpsych PDFDocument27 pagesSe 04 Abpsych PDFBea SengcoNo ratings yet
- DSM 5 IntroductionDocument25 pagesDSM 5 Introductionjagdish_vankar100% (2)
- Clinical Interview and ObservationDocument47 pagesClinical Interview and Observationmlssmnn100% (1)
- Understanding Psychological AbnormalityDocument21 pagesUnderstanding Psychological AbnormalityTitikshaNo ratings yet
- Introduction To DSM 5 2Document61 pagesIntroduction To DSM 5 2denfan100% (1)
- 2 Year Physical Therapy NotesDocument129 pages2 Year Physical Therapy Notesthwiseman94% (17)
- DSM 5 Mood DisorderDocument9 pagesDSM 5 Mood DisorderErlin IrawatiNo ratings yet
- The Pharmacists Guide To Antimicrobial Therapy and StewardshipDocument244 pagesThe Pharmacists Guide To Antimicrobial Therapy and StewardshipAyman Khalil100% (1)
- AMC MCQ Recalls 2017Document2 pagesAMC MCQ Recalls 2017prepengo90% (10)
- Care For Elderly - TAGALOGDocument29 pagesCare For Elderly - TAGALOGKarl Kevin MarbellaNo ratings yet
- Psychological AssessmentDocument227 pagesPsychological AssessmentBea SengcoNo ratings yet
- Clinical PsychDocument13 pagesClinical PsychJESSA MAVEL VELORIANo ratings yet
- Use of The Manual ChapterDocument34 pagesUse of The Manual ChapterSheemaNo ratings yet
- 1diagnosis and Classification in PsychiatryDocument77 pages1diagnosis and Classification in PsychiatryTuwilikaNafukaNo ratings yet
- Classification SystemsDocument14 pagesClassification Systemscinnabon9.75No ratings yet
- DSM 5Document2 pagesDSM 5Alberto Preciado100% (1)
- Clinical Assessment, Diagnosis and Treatment GuideDocument7 pagesClinical Assessment, Diagnosis and Treatment GuideLizana PamittanNo ratings yet
- Diagnostic ToolsDocument9 pagesDiagnostic Toolssilaemoo2002No ratings yet
- Classification Systems TextDocument4 pagesClassification Systems TextKinjal KoliNo ratings yet
- Dsm-Iv & 5Document18 pagesDsm-Iv & 5strioagung06No ratings yet
- SPMM Notes Paper ADocument572 pagesSPMM Notes Paper AKanaga6432No ratings yet
- AssignmentDocument9 pagesAssignmentIshita AdhikariNo ratings yet
- Behavioural Disorder AnswerDocument7 pagesBehavioural Disorder Answerdipayan bhattacharyaNo ratings yet
- The Future Arrived: ViewpointDocument2 pagesThe Future Arrived: ViewpointDaniela Ocampo BoteroNo ratings yet
- Patho 1 CIA 1ADocument14 pagesPatho 1 CIA 1APranjal SuranaNo ratings yet
- DiagnosisDocument59 pagesDiagnosisRizky KykyNo ratings yet
- Feighner Et Al (1972) - Diagnostic Criteria For Use in Psychiatric ResearchDocument7 pagesFeighner Et Al (1972) - Diagnostic Criteria For Use in Psychiatric ResearchEmily RedmanNo ratings yet
- Part 1. Approach To The PatientDocument23 pagesPart 1. Approach To The PatientKyra RMNo ratings yet
- Proposed Definitions of Abnormal Behavior?Document7 pagesProposed Definitions of Abnormal Behavior?Jay Mark CabreraNo ratings yet
- Clinical Assessment and Diagnosis GuideDocument25 pagesClinical Assessment and Diagnosis GuideRullita Aristya MNo ratings yet
- APA - DSM 5 Section III PDFDocument3 pagesAPA - DSM 5 Section III PDFraluca_ghigaNo ratings yet
- Diagnosis and AssessmentDocument10 pagesDiagnosis and AssessmentcynthiasenNo ratings yet
- Differentiating Somatoform Disorder, Factitious Disorder and MalingeringDocument33 pagesDifferentiating Somatoform Disorder, Factitious Disorder and MalingeringwimpyyNo ratings yet
- Clinical psychology basicsDocument19 pagesClinical psychology basicsviji sathishNo ratings yet
- DSM-5 Classification OverviewDocument75 pagesDSM-5 Classification OverviewtincruzNo ratings yet
- AbnmlDocument4 pagesAbnmlnandana remananNo ratings yet
- Lecture 2 Psychiatric Diagnoses SlidesDocument33 pagesLecture 2 Psychiatric Diagnoses Slidesmichelle.hoNo ratings yet
- NCM 117 Rle - DSM - Iv TR and DSM - VDocument6 pagesNCM 117 Rle - DSM - Iv TR and DSM - VKate Angelique RodriguezNo ratings yet
- Mild Neurocognitive Disorder Fact Sheet PDFDocument1 pageMild Neurocognitive Disorder Fact Sheet PDFAle M. MartinezNo ratings yet
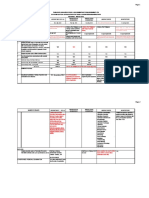
- Validity of Psychiatric DisordersDocument36 pagesValidity of Psychiatric DisordersAteev ChandnaNo ratings yet
- Psychological Assessment in Different Setting - PsychologicalDocument7 pagesPsychological Assessment in Different Setting - PsychologicalKian LaNo ratings yet
- Unit 1 - Understanding PsychopathologyDocument6 pagesUnit 1 - Understanding Psychopathologybiyaspsy9No ratings yet
- Introduction To Psychopathology Book NotesDocument35 pagesIntroduction To Psychopathology Book NotesZohaib Ahmad100% (1)
- Chapter5Document42 pagesChapter5peachypeachyNo ratings yet
- Bishakha Acharya (Abnormal Psychology)Document7 pagesBishakha Acharya (Abnormal Psychology)bishakha stylesNo ratings yet
- Eunice Report SumamryDocument6 pagesEunice Report SumamryRoxanne LoberesNo ratings yet
- DSM V Intelectual DissabilitiesDocument130 pagesDSM V Intelectual DissabilitiesYarelis Montero MercadoNo ratings yet
- Essay On DSM-5Document2 pagesEssay On DSM-5Rameesha MalikNo ratings yet
- Se 07 Abpsych PDFDocument45 pagesSe 07 Abpsych PDFBea SengcoNo ratings yet
- Se 05 Abpsych PDFDocument28 pagesSe 05 Abpsych PDFBea SengcoNo ratings yet
- History, Theories and Paradigms in Abnormal PsychologyDocument29 pagesHistory, Theories and Paradigms in Abnormal PsychologyBea SengcoNo ratings yet
- Se 01 Abpsych PDFDocument28 pagesSe 01 Abpsych PDFBea SengcoNo ratings yet
- PRC List of RequirementsDocument24 pagesPRC List of RequirementscharmainegoNo ratings yet
- GeishaDocument1 pageGeishaBea SengcoNo ratings yet
- I Remembered That Day Again, The Day You Express Your Love It's Such A Beauty in My Eyes, That Red Heart-Shaped NecklaceDocument1 pageI Remembered That Day Again, The Day You Express Your Love It's Such A Beauty in My Eyes, That Red Heart-Shaped NecklaceBea SengcoNo ratings yet
- List of Most Common Usmle DiseasesDocument3 pagesList of Most Common Usmle Diseasesantoine sioufiNo ratings yet
- Coding With Meddra f2f CourseDocument54 pagesCoding With Meddra f2f CoursetudorNo ratings yet
- ChickenpoxDocument2 pagesChickenpoxNorhana LangiNo ratings yet
- 1 +Theresia+Jamini+1-9Document9 pages1 +Theresia+Jamini+1-9Florentina yohana ngeluNo ratings yet
- Student SYB: Chet Cunha MS IV January 22, 2009Document15 pagesStudent SYB: Chet Cunha MS IV January 22, 2009okarasemNo ratings yet
- Ovarian Cancer Antigen (Ca-125) : Enzyme Immunoassay Test Kit Catalog Number: 10103Document2 pagesOvarian Cancer Antigen (Ca-125) : Enzyme Immunoassay Test Kit Catalog Number: 10103yousrazeidan1979No ratings yet
- All by Gyn Obst Depart PDFDocument27 pagesAll by Gyn Obst Depart PDFRaouf Ra'fat Soliman100% (2)
- HEALTH QUESTIONNAIRE (Talatanungan Ukol Sa Kalusugan) :: Please Read Carefully (Basahin NG Mabuti)Document2 pagesHEALTH QUESTIONNAIRE (Talatanungan Ukol Sa Kalusugan) :: Please Read Carefully (Basahin NG Mabuti)Karen Kaye PasamonteNo ratings yet
- ONF mTBI Guidelines 2nd Edition COMPLETE PDFDocument85 pagesONF mTBI Guidelines 2nd Edition COMPLETE PDFMarina SwansonNo ratings yet
- Morphology Morphology: Gross: White, Chalky Fat NecrosisDocument50 pagesMorphology Morphology: Gross: White, Chalky Fat NecrosisJc GaldosNo ratings yet
- Animal Bite: Pablo R. Quedado, MDDocument36 pagesAnimal Bite: Pablo R. Quedado, MDPrincess Noreen SavellanoNo ratings yet
- Wellness Massage LectureDocument19 pagesWellness Massage LectureScytheNo ratings yet
- Appoach To Brittle Diabetes: Clinical Algorithm To Determine The EtiologyDocument2 pagesAppoach To Brittle Diabetes: Clinical Algorithm To Determine The EtiologyMudassar SattarNo ratings yet
- Mnemonic SDocument3 pagesMnemonic SRohini SelvarajahNo ratings yet
- Squamous Papilloma On Hard Palate: Case Report and Literature ReviewDocument3 pagesSquamous Papilloma On Hard Palate: Case Report and Literature ReviewadelNo ratings yet
- Blood in StoolDocument3 pagesBlood in StoolRae RayNo ratings yet
- Philippine National Police Regional Health Service Ncrpo Physical Examination Guide For Annual Physical Examination (APE)Document2 pagesPhilippine National Police Regional Health Service Ncrpo Physical Examination Guide For Annual Physical Examination (APE)james antonioNo ratings yet
- CT Public v82 8 9Document2 pagesCT Public v82 8 9Dida HermaNo ratings yet
- YOGA AND DIGESTION and ELIMINATION1Document25 pagesYOGA AND DIGESTION and ELIMINATION1Toby SmallNo ratings yet
- Neonatal ObservationsDocument3 pagesNeonatal ObservationsMuhammad Bayu Zohari HutagalungNo ratings yet
- 10 Scientifically Proven Health Benefits of Taking A BathDocument6 pages10 Scientifically Proven Health Benefits of Taking A BathKiara Isabel Dela VegaNo ratings yet
- Cause of Death - 98Document18 pagesCause of Death - 98Suhrud PanchawaghNo ratings yet