You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- 485 1230 1 PB PDFDocument9 pages485 1230 1 PB PDFTri HandayaniNo ratings yet
- 2 Vol. 4 Issue 12 December 2013 IJPSR 1114 Paper 2Document11 pages2 Vol. 4 Issue 12 December 2013 IJPSR 1114 Paper 2Hepy PutraNo ratings yet
- 446 1255 1 PB PDFDocument12 pages446 1255 1 PB PDFToni HudaNo ratings yet
- 492 1241 1 PBDocument6 pages492 1241 1 PBAnonymous dkEBxwVJONo ratings yet
- 2 Vol. 4 Issue 12 December 2013 IJPSR 1114 Paper 2Document11 pages2 Vol. 4 Issue 12 December 2013 IJPSR 1114 Paper 2Hepy PutraNo ratings yet
- A Systematic Review of Strategies To Prevent Cisplatin-Induced NephrotoxicityDocument11 pagesA Systematic Review of Strategies To Prevent Cisplatin-Induced NephrotoxicityTri HandayaniNo ratings yet
- Diare Epidemic in Senden HamletDocument10 pagesDiare Epidemic in Senden HamletDheaDesniaNo ratings yet
- 1 PBDocument7 pages1 PBTri HandayaniNo ratings yet
- Hnavfup ProtocolDocument5 pagesHnavfup ProtocolTri HandayaniNo ratings yet
- Kekurangan Vitamin A Pada Kelompok Bay1 Dan Faktor Yang Berhubungan DL Kabupaten BogorDocument7 pagesKekurangan Vitamin A Pada Kelompok Bay1 Dan Faktor Yang Berhubungan DL Kabupaten BogorTri HandayaniNo ratings yet
- Pharmacoeconomics: Costs and Consequences of Treatment AlternativesDocument18 pagesPharmacoeconomics: Costs and Consequences of Treatment AlternativesTri HandayaniNo ratings yet
- Strawberry leaves extract antioxidant and sunscreen activitiesDocument6 pagesStrawberry leaves extract antioxidant and sunscreen activitiesTri HandayaniNo ratings yet
- Brazilian Hypertension Guideline Recommends BP Targets for Kidney DiseaseDocument5 pagesBrazilian Hypertension Guideline Recommends BP Targets for Kidney DiseaseTri HandayaniNo ratings yet
- Guidline OndansentronDocument5 pagesGuidline OndansentronTri HandayaniNo ratings yet
- Optimizing Polymers in Piroxicam Ocusert for Controlled Drug ReleaseDocument10 pagesOptimizing Polymers in Piroxicam Ocusert for Controlled Drug ReleaseTri HandayaniNo ratings yet
- 1 53752 1 10 20170125Document10 pages1 53752 1 10 20170125Tri HandayaniNo ratings yet
- Journal of Pharmaceutical and Biomedical Analysis Volume 125 Issue 2016 (Doi 10.1016/j.jpba.2016.03.024) Abdallah, Inas A. Hammell, Dana C. Hassan, Hazem E. Stinchcom - Norelgestromin - Ethinyl eDocument9 pagesJournal of Pharmaceutical and Biomedical Analysis Volume 125 Issue 2016 (Doi 10.1016/j.jpba.2016.03.024) Abdallah, Inas A. Hammell, Dana C. Hassan, Hazem E. Stinchcom - Norelgestromin - Ethinyl eTri HandayaniNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- NSK 2013 A00-000-001 enDocument26 pagesNSK 2013 A00-000-001 enThato Merapelo PuleNo ratings yet
- Self-Esteem Disturbance: Submitted To: Ma'am Sadia Kanwal Submitted By: Fatima AzharDocument15 pagesSelf-Esteem Disturbance: Submitted To: Ma'am Sadia Kanwal Submitted By: Fatima AzharbinteazharNo ratings yet
- Systemic Diseases and Their Management for ProsthodontistsDocument5 pagesSystemic Diseases and Their Management for ProsthodontistssyamNo ratings yet
- Sensory Deprivation and Loss-4Document32 pagesSensory Deprivation and Loss-4Scott Daniel Phillips100% (1)
- Reimbursement Claim FormDocument3 pagesReimbursement Claim FormGanesh Kumar100% (1)
- Ann BibDocument5 pagesAnn Bibapi-317311486No ratings yet
- Research Updates - Homeopathy Vol 7 Issue 3 - Special Edition - Priority Areas For Research in HomeopathyDocument32 pagesResearch Updates - Homeopathy Vol 7 Issue 3 - Special Edition - Priority Areas For Research in HomeopathySaurav AroraNo ratings yet
- Understanding SmaDocument40 pagesUnderstanding SmaThanos ZihnalisNo ratings yet
- 2018 DPRI Booklet As of February 2019Document34 pages2018 DPRI Booklet As of February 2019kkabness101 YULNo ratings yet
- Nursing Care PlanDocument26 pagesNursing Care PlanNeil Anthony78% (18)
- Peds PresentationDocument31 pagesPeds Presentationapi-247218432No ratings yet
- Orange County Pact 14 06Document18 pagesOrange County Pact 14 06api-22559015No ratings yet
- Proquest Research Library Health and MedicineDocument1,290 pagesProquest Research Library Health and MedicineIng Mauricio SabogalNo ratings yet
- PSG202 - 25 - A Complete Guide To Therapy - Kove, J - Cap 16 - PP 247-259Document8 pagesPSG202 - 25 - A Complete Guide To Therapy - Kove, J - Cap 16 - PP 247-259oswaldoNo ratings yet
- Dermnet NZ: MelasmaDocument5 pagesDermnet NZ: MelasmaWin TheinNo ratings yet
- Children's Hospital of Eastern Ontario Pain Scale (CHEOPS)Document3 pagesChildren's Hospital of Eastern Ontario Pain Scale (CHEOPS)Nick O NeillNo ratings yet
- Nutrition in The Critically Ill PatientDocument13 pagesNutrition in The Critically Ill PatientnainazahraNo ratings yet
- Botox G Art 2016Document13 pagesBotox G Art 2016Anamaria ZaccoloNo ratings yet
- Dialysis Power PointDocument20 pagesDialysis Power PointJor GarciaNo ratings yet
- Joella Pregnancy Support GroupDocument2 pagesJoella Pregnancy Support GroupElle ctrica100% (2)
- Camptodactyly: Christian Dumontier MD, PHD Centre de La Main Guadeloupe - FwiDocument49 pagesCamptodactyly: Christian Dumontier MD, PHD Centre de La Main Guadeloupe - FwiProfesseur Christian Dumontier100% (1)
- NDT 45697 Efficacy of Second Generation Antipsychotics in Patients at 061813Document8 pagesNDT 45697 Efficacy of Second Generation Antipsychotics in Patients at 061813twahyuningsih_16No ratings yet
- TP BookletDocument12 pagesTP BookletAkino InuiNo ratings yet
- Cobalt 60 VS Iridium 192Document6 pagesCobalt 60 VS Iridium 192Rares PNo ratings yet
- Chapter 1 - Psychology As A ScienceDocument21 pagesChapter 1 - Psychology As A Sciencevarunas_250% (2)
- Clostridium Difficile Infection Fidaxomicin Esnm1Document11 pagesClostridium Difficile Infection Fidaxomicin Esnm1Pet UrNo ratings yet
- Glutathione and Its Antiaging and Antimelanogenic EffectsDocument7 pagesGlutathione and Its Antiaging and Antimelanogenic EffectsG. I.No ratings yet
- Tabela Grifo LaboratoryDocument11 pagesTabela Grifo LaboratoryGRIFO DIVULGA100% (2)
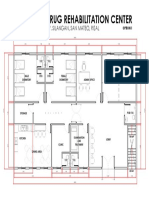
- Proposed Drug Rehabilitation Center: Monterey Sudb., Brgy. Silangan, San Mateo, RizalDocument1 pageProposed Drug Rehabilitation Center: Monterey Sudb., Brgy. Silangan, San Mateo, RizalJonathan MazonNo ratings yet
- Revised Case Report - HemorrhoidsDocument47 pagesRevised Case Report - Hemorrhoidschristina_love08100% (2)