You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Mental Illness Attitude Scale (Modified OMICC QuestionnaireDocument6 pagesMental Illness Attitude Scale (Modified OMICC QuestionnaireSyed Faizan100% (7)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Treatment of Anxiety Disorders Clinician Guides and Patient ManualsDocument624 pagesThe Treatment of Anxiety Disorders Clinician Guides and Patient Manualsladylife100% (11)
- Motorcycle DiariesDocument9 pagesMotorcycle DiariesGelo De Guzman100% (1)
- DiarrheaDocument24 pagesDiarrheaash ashNo ratings yet
- Obesity Exercise PrescriptionDocument34 pagesObesity Exercise Prescriptionkhushbu88% (8)
- IntroductiontoEpidemiologyandPublicHealth AnswersDocument17 pagesIntroductiontoEpidemiologyandPublicHealth AnswersDiamond_136100% (2)
- History of MicrobiologyDocument3 pagesHistory of MicrobiologyAngeli ButedNo ratings yet
- Obpp 3 - AetDocument86 pagesObpp 3 - AetAshley ThaynNo ratings yet
- Artifact #2Document16 pagesArtifact #2Ashley ThaynNo ratings yet
- Obpp 3 - AetDocument85 pagesObpp 3 - AetAshley ThaynNo ratings yet
- Occupation-Based Life-Skills Program For Incarcerated Women: A Literature ReviewDocument14 pagesOccupation-Based Life-Skills Program For Incarcerated Women: A Literature ReviewAshley ThaynNo ratings yet
- Artifact #7Document13 pagesArtifact #7Ashley ThaynNo ratings yet
- Artifact #5Document2 pagesArtifact #5Ashley ThaynNo ratings yet
- Artifact #6Document40 pagesArtifact #6Ashley ThaynNo ratings yet
- Running Head: Budgeting Program For Incarcerated Women 1Document26 pagesRunning Head: Budgeting Program For Incarcerated Women 1Ashley ThaynNo ratings yet
- Artifact #4bDocument2 pagesArtifact #4bAshley ThaynNo ratings yet
- Artifact #1Document12 pagesArtifact #1Ashley ThaynNo ratings yet
- Artifact #4cDocument2 pagesArtifact #4cAshley ThaynNo ratings yet
- mCIMT Is Less Intense Than CIMT But Still Incorporates The Same Principle Demanding Less Intensity and Time ThanDocument4 pagesmCIMT Is Less Intense Than CIMT But Still Incorporates The Same Principle Demanding Less Intensity and Time ThanAshley ThaynNo ratings yet
- Artifact #3Document3 pagesArtifact #3Ashley ThaynNo ratings yet
- Artifact #2bDocument11 pagesArtifact #2bAshley ThaynNo ratings yet
- Artifact #2aDocument9 pagesArtifact #2aAshley ThaynNo ratings yet
- Depression in Today - BioDocument5 pagesDepression in Today - Bioapi-272648963No ratings yet
- Archives of Gerontology and GeriatricsDocument7 pagesArchives of Gerontology and GeriatricsAna ArhipNo ratings yet
- PDF Created With Pdffactory Pro Trial Version: Page 1 of 3Document3 pagesPDF Created With Pdffactory Pro Trial Version: Page 1 of 3HindNo ratings yet
- Chapter 3 PsychDocument12 pagesChapter 3 Psychred_gyrl9282No ratings yet
- Staph and Strep Lab Report BMS 501Document2 pagesStaph and Strep Lab Report BMS 501aruiz93No ratings yet
- Occupational Therapy Rehabilitation Paraplegic PatientDocument7 pagesOccupational Therapy Rehabilitation Paraplegic PatientAlina PasăreNo ratings yet
- Documentation: Siji M. SunnyDocument5 pagesDocumentation: Siji M. SunnySUNNY__SIJINo ratings yet
- Presentations Sux ApnoeaDocument18 pagesPresentations Sux ApnoeaalishbaNo ratings yet
- Apotex Pharmachem Product ListDocument2 pagesApotex Pharmachem Product Listমোঃ এমদাদুল হকNo ratings yet
- Forearm Fracture in ChildrenDocument45 pagesForearm Fracture in ChildrenMagnusNo ratings yet
- Permission To Attend Hockey DayDocument4 pagesPermission To Attend Hockey Dayapi-244287783No ratings yet
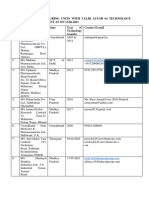
- List of Manufacturing Units With Valid Ayush 64 Technology Transfer Agreement As On 15.06.2021Document5 pagesList of Manufacturing Units With Valid Ayush 64 Technology Transfer Agreement As On 15.06.2021Sunira EnterprisesNo ratings yet
- Review of Literature: MorphologyDocument38 pagesReview of Literature: MorphologyVaishu Gunalan0% (1)
- PhobiasDocument10 pagesPhobiasapi-276690632No ratings yet
- Keeler Ophthalmoscope Bulb and Retinoscope Bulb ModelsDocument1 pageKeeler Ophthalmoscope Bulb and Retinoscope Bulb ModelsEDRAES17No ratings yet
- Diatermo MB 122 and MB 160 Mono-Bipolar: Cautery & ElectrosurgeryDocument13 pagesDiatermo MB 122 and MB 160 Mono-Bipolar: Cautery & ElectrosurgeryDani Daniela100% (1)
- Cognitv EmphatyDocument6 pagesCognitv EmphatyAndrea MenesesNo ratings yet
- FISIOGRAFT ENG Set 17 PDFDocument28 pagesFISIOGRAFT ENG Set 17 PDFmaxNo ratings yet
- Legumes - AnOverview PDFDocument6 pagesLegumes - AnOverview PDFMayuri JagtapNo ratings yet
- Book Club Guide: INVINCIBLEDocument1 pageBook Club Guide: INVINCIBLEEpicReadsNo ratings yet
- Dissertation Topics 2Document21 pagesDissertation Topics 2Apollo Institute of Hospital Administration100% (1)
- Hemorragic Post PartumDocument10 pagesHemorragic Post PartumJihan NurlailaNo ratings yet
- Class 11 English Snapshots Chapter 7Document2 pagesClass 11 English Snapshots Chapter 7Alpha StarNo ratings yet