You might also like
- Stereotactic Radiosurgery and Stereotactic Body Radiation Therapy: A Comprehensive GuideFrom EverandStereotactic Radiosurgery and Stereotactic Body Radiation Therapy: A Comprehensive GuideDaniel M. TrifilettiNo ratings yet
- Signs and Symptoms of TMJ Disorders in Adults After Adolescent Herbst Therapy: A 6-Year and 32-Year Radiographic and Clinical Follow-Up StudyDocument14 pagesSigns and Symptoms of TMJ Disorders in Adults After Adolescent Herbst Therapy: A 6-Year and 32-Year Radiographic and Clinical Follow-Up StudyDr Kiara KirpalaniNo ratings yet
- Repetitive Transcranial Magnetic Stimulation Treatment for Depressive Disorders: A Practical GuideFrom EverandRepetitive Transcranial Magnetic Stimulation Treatment for Depressive Disorders: A Practical GuideNo ratings yet
- Abnormalities of Masseter Reflex InhibitoryDocument5 pagesAbnormalities of Masseter Reflex InhibitoryAndres Rojas JerezNo ratings yet
- Head Gear Effect - PancherzDocument11 pagesHead Gear Effect - PancherzSrishti SyalNo ratings yet
- The Expression of MDM2/CDK4 Gene Product in The Differential Diagnosis of Well Differentiated Liposarcoma and Large Deep-Seated LipomaDocument5 pagesThe Expression of MDM2/CDK4 Gene Product in The Differential Diagnosis of Well Differentiated Liposarcoma and Large Deep-Seated LipomaaslinNo ratings yet
- HerbstDocument17 pagesHerbstLudy Jiménez ValdiviaNo ratings yet
- Ocr 12416Document7 pagesOcr 12416khaled mohammadNo ratings yet
- The Journal of Prosthetic Dentistry Volume 49 Issue 4 1983 (Doi 10.1016 - 0022-3913 (83) 90318-9) Lawrence A. Weinberg - The Role of Stress, Occlusion, and Condyle Position in TMJ Dysfunction-PainDocument14 pagesThe Journal of Prosthetic Dentistry Volume 49 Issue 4 1983 (Doi 10.1016 - 0022-3913 (83) 90318-9) Lawrence A. Weinberg - The Role of Stress, Occlusion, and Condyle Position in TMJ Dysfunction-PainMichaelAndreasNo ratings yet
- Cranifaringioma 1Document13 pagesCranifaringioma 1Oka Iramda SaputraNo ratings yet
- Imaging Manifestations of Spinal Fractures in Ankylosing SpondylitisDocument10 pagesImaging Manifestations of Spinal Fractures in Ankylosing SpondylitisEkaNo ratings yet
- Aggressive Periodontitis inDocument5 pagesAggressive Periodontitis inOctavian CiceuNo ratings yet
- Disk Displacement, Eccentric Condylar Position, OsteoarthrosisDocument10 pagesDisk Displacement, Eccentric Condylar Position, OsteoarthrosisAlejandro RuizNo ratings yet
- Battagel 1991Document11 pagesBattagel 1991LanaNo ratings yet
- The Characteristics of Scoliosis in Prader-Willi Syndrome (PWS) : Analysis of 58 Scoliosis Patients With PWSDocument6 pagesThe Characteristics of Scoliosis in Prader-Willi Syndrome (PWS) : Analysis of 58 Scoliosis Patients With PWSsalvatore balzanoNo ratings yet
- Artigo Comparação Botox e DyportDocument5 pagesArtigo Comparação Botox e DyportGabriela IesNo ratings yet
- Temporomandibular: Joint Displacement Without ReductionDocument5 pagesTemporomandibular: Joint Displacement Without ReductionleandrariosllNo ratings yet
- The Importance of Flap Design in Third Molar Surgery: A Systematic ReviewDocument6 pagesThe Importance of Flap Design in Third Molar Surgery: A Systematic ReviewSaif HashimNo ratings yet
- Panc Herz 1999Document8 pagesPanc Herz 1999libroscasitaNo ratings yet
- Long-Term Effects of The Herbst Appliance On The Dental Arches and Arch Relationships: A Biometric StudyDocument13 pagesLong-Term Effects of The Herbst Appliance On The Dental Arches and Arch Relationships: A Biometric StudyIvan Rivero MarquezNo ratings yet
- Poster SMA Gene Therapy CBN 2022Document1 pagePoster SMA Gene Therapy CBN 2022Rodrigo HolandaNo ratings yet
- Luzi 2013Document6 pagesLuzi 2013Rohit K ChouguleNo ratings yet
- Arthroscopic Drilling For The Treatment of Osteochondral Lesions of The TalusDocument7 pagesArthroscopic Drilling For The Treatment of Osteochondral Lesions of The TalusAnonymous kdBDppigENo ratings yet
- 5 6201509562231555914Document7 pages5 6201509562231555914Rahul ReddyNo ratings yet
- CrossbowDocument11 pagesCrossbowm.malekiNo ratings yet
- Gibas Et Al. - A Possible Specific Chromosome Change in Transitional Cell Carcinoma of The BladderDocument10 pagesGibas Et Al. - A Possible Specific Chromosome Change in Transitional Cell Carcinoma of The BladderyuenkeithNo ratings yet
- Three-Dimensional Hard Tissue Palatal Size and Shape: A 10-Year Longitudinal Evaluation in Healthy AdultsDocument14 pagesThree-Dimensional Hard Tissue Palatal Size and Shape: A 10-Year Longitudinal Evaluation in Healthy AdultsSankhya100% (1)
- 2010niko Christian BockDocument6 pages2010niko Christian BockNeeraj AroraNo ratings yet
- Predição Da Estabilidade Trata MesioclusãoDocument7 pagesPredição Da Estabilidade Trata MesioclusãomargarethNo ratings yet
- Faktor Prognosis PonsDocument9 pagesFaktor Prognosis PonsindanazulfaaNo ratings yet
- JTD 08 10 E1136Document14 pagesJTD 08 10 E1136Yacine Tarik AizelNo ratings yet
- Mycosphere 8 6 7Document8 pagesMycosphere 8 6 7Teodoro Chivatá BedoyaNo ratings yet
- Cadera ActivaciónDocument5 pagesCadera ActivaciónDavid Aliaga GordilloNo ratings yet
- Articulo 9Document7 pagesArticulo 9Daniela NarváezNo ratings yet
- Primary Pseudomyogenic Hemangioendothelioma of RightDocument10 pagesPrimary Pseudomyogenic Hemangioendothelioma of RightAndres Mera VergaraNo ratings yet
- The Boxer's Fracture: Splint Immobilization Is Not NecessaryDocument5 pagesThe Boxer's Fracture: Splint Immobilization Is Not NecessarySandy Tama Okvan YudhaNo ratings yet
- Accepted Manuscript: The Spine JournalDocument30 pagesAccepted Manuscript: The Spine JournalCarlos RiveraNo ratings yet
- PIIS0889540606004471Document2 pagesPIIS0889540606004471Evelin CastilloNo ratings yet
- Terceros y Segundos MolaresDocument10 pagesTerceros y Segundos MolaresROMÁN RUIZNo ratings yet
- Structure and Function of The Temporomandibular Joint Disc: Implications For Tissue EngineeringDocument13 pagesStructure and Function of The Temporomandibular Joint Disc: Implications For Tissue EngineeringMaria Beatriz Solis ValenciaNo ratings yet
- Lecture 16 2Document6 pagesLecture 16 2dayane2394No ratings yet
- MRI Analysis Shows Effectiveness of Michigan Splint Therapy for TMJ DiscsDocument8 pagesMRI Analysis Shows Effectiveness of Michigan Splint Therapy for TMJ Discsluis alejandroNo ratings yet
- J Joms 2008 01 046Document10 pagesJ Joms 2008 01 046Delta JackNo ratings yet
- Tendon Transfer For Upper Level Brachial Plexus InjuryDocument22 pagesTendon Transfer For Upper Level Brachial Plexus InjuryreyNo ratings yet
- Longterm Treatment Effects of The FR2Document6 pagesLongterm Treatment Effects of The FR2Fabian BarretoNo ratings yet
- Expansion RapidaDocument11 pagesExpansion RapidaNayely MiguelNo ratings yet
- AnaetDocument4 pagesAnaethidrisdmnk_747467972No ratings yet
- A Systematic Review On The Association Between Clinical Symptoms and CBCT Findings in Symptomatic TMJ Degenerative Joint DiseaseDocument14 pagesA Systematic Review On The Association Between Clinical Symptoms and CBCT Findings in Symptomatic TMJ Degenerative Joint DiseaseNado CuiabáNo ratings yet
- Eficacia de La ErupciónForzada2Document11 pagesEficacia de La ErupciónForzada2Francisco Javier Mardones QuintanillaNo ratings yet
- Jurnal Zygomatic 2013Document7 pagesJurnal Zygomatic 2013Defri ChanNo ratings yet
- Indirect Measurement of The Temporomandibular Joint Disc Elasticity With Magnetic Resonance ImagingDocument7 pagesIndirect Measurement of The Temporomandibular Joint Disc Elasticity With Magnetic Resonance ImagingguhanderNo ratings yet
- Distal Radius Fractures With Ulnar Styloid Fracture - V2Document30 pagesDistal Radius Fractures With Ulnar Styloid Fracture - V2Chinmaye PurushothamNo ratings yet
- Activator HeadgearDocument9 pagesActivator HeadgearThendral DevanathanNo ratings yet
- Treatment and Posttreatment Effects Induced by The Forsus Appliance A Controlled Clinical StudyDocument8 pagesTreatment and Posttreatment Effects Induced by The Forsus Appliance A Controlled Clinical Studyorthodonticlit orthodonticlitNo ratings yet
- HerbstDocument12 pagesHerbstEfrein Ticona HilasacaNo ratings yet
- Comparison of Porous vs Non-Porous Teflon Membranes for Treating Class II Furcation DefectsDocument8 pagesComparison of Porous vs Non-Porous Teflon Membranes for Treating Class II Furcation DefectsSebastián BernalNo ratings yet
- Ossiculoplasty: Autograft VS AllograftDocument6 pagesOssiculoplasty: Autograft VS AllograftIJAR JOURNALNo ratings yet
- J Jds 2020 05 016Document5 pagesJ Jds 2020 05 016Kim Chi NguyễnNo ratings yet
- Articulo Clase IIIDocument8 pagesArticulo Clase IIIMary ViloriaNo ratings yet
- Hoz2020, Tce Botella, Gas LacrimogenoDocument5 pagesHoz2020, Tce Botella, Gas LacrimogenoAlberto GutierrezNo ratings yet
- Anexo 55 Lamina M15 Peligros Por GranizadaDocument1 pageAnexo 55 Lamina M15 Peligros Por GranizadaBryan Yufra OchoaNo ratings yet
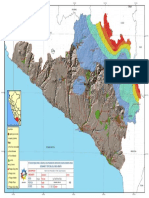
- Anexo 55 Lamina M1 Peligros Por SismosDocument1 pageAnexo 55 Lamina M1 Peligros Por SismosBryan Yufra OchoaNo ratings yet
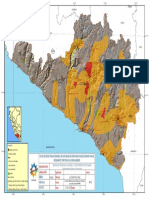
- Anexo 55 Lamina M13 Peligros Erosion Lateral y Mvto MasasDocument1 pageAnexo 55 Lamina M13 Peligros Erosion Lateral y Mvto MasasBryan Yufra OchoaNo ratings yet
- Anexo 55 Lamina M2 Peligros Por TsunamisDocument1 pageAnexo 55 Lamina M2 Peligros Por TsunamisBryan Yufra OchoaNo ratings yet
- Mr. Abhishek Sharma-1Document3 pagesMr. Abhishek Sharma-1Abhishek SharmaNo ratings yet
- Parts of The Body and Health ProblemDocument13 pagesParts of The Body and Health ProblemSonia Tri AgustinaNo ratings yet
- Enhanced Massage Therapy NC2 - POLODocument39 pagesEnhanced Massage Therapy NC2 - POLORussiel DagohoyNo ratings yet
- JciDocument5 pagesJcialfredsamuelNo ratings yet
- PTSD EssayDocument2 pagesPTSD Essayapi-335023853No ratings yet
- Ischemic Heart Disease 19.9.90Document27 pagesIschemic Heart Disease 19.9.90Hamidreza GoodarzynejadNo ratings yet
- Conversion de Anestesia Espinal A General en Apendicectomia AbiertaDocument1 pageConversion de Anestesia Espinal A General en Apendicectomia AbiertaJavier WebarNo ratings yet
- Physical Health Assessment PreparationDocument3 pagesPhysical Health Assessment PreparationaliNo ratings yet
- CPG - Management of AcneDocument97 pagesCPG - Management of Acneumiraihana1No ratings yet
- 2005-4144s1 04 Nipper-Hemodialysis OverviewDocument19 pages2005-4144s1 04 Nipper-Hemodialysis Overviewsaleh1978No ratings yet
- Medicare Policy: The Independent Payment Advisory Board: A New Approach To Controlling Medicare SpendingDocument24 pagesMedicare Policy: The Independent Payment Advisory Board: A New Approach To Controlling Medicare SpendingCatherine SnowNo ratings yet
- Brenda MilnerDocument8 pagesBrenda Milneryuritrujillo33No ratings yet
- Practice TestDocument6 pagesPractice TestJulie May SuganobNo ratings yet
- Pid Casestudy 2014 PDFDocument4 pagesPid Casestudy 2014 PDFNur Syamsiah MNo ratings yet
- Community and Public Health Nursing DifferencesDocument1 pageCommunity and Public Health Nursing DifferencesAnnalisa Telles100% (2)
- NTSB LIRR ReportDocument26 pagesNTSB LIRR ReportNewsdayNo ratings yet
- Recycling Banks To Reduce Scavenging at Dumps in Lagos, NigeriaDocument11 pagesRecycling Banks To Reduce Scavenging at Dumps in Lagos, NigeriaMary NgbakoNo ratings yet
- Critical Care Infection ControlDocument41 pagesCritical Care Infection ControlMisbah 114No ratings yet
- 256 CircumcisionDocument5 pages256 CircumcisionMD Luthfy LubisNo ratings yet
- Basic Life SupportDocument9 pagesBasic Life Supportaina_boydonNo ratings yet
- Disease Symptoms and Patient Profile DatasetDocument6 pagesDisease Symptoms and Patient Profile Datasetnavyalohitha49No ratings yet
- NCP-S/P AppendectomyDocument6 pagesNCP-S/P Appendectomytinatin989100% (7)
- Project Proposal 5 28 19Document5 pagesProject Proposal 5 28 19api-461464117No ratings yet
- The ShelfDocument18 pagesThe Shelfsowcowdd100% (5)
- Facts and Definition of EclampsiaDocument5 pagesFacts and Definition of EclampsiaChoi Gong JuNo ratings yet
- Treatment Aspects in Perioperative NursingDocument51 pagesTreatment Aspects in Perioperative NursingShibin Jacob100% (2)
- Collecting Objective DataDocument61 pagesCollecting Objective DataAdrianAripNo ratings yet
- The Art and Science of Homeopathic Case TakingDocument162 pagesThe Art and Science of Homeopathic Case Takingmihaipopescu0No ratings yet
- Cervical Spine CYRIAXDocument16 pagesCervical Spine CYRIAXCarlos TavaresNo ratings yet
- OB MedsDocument19 pagesOB Medsohsnapitslei100% (2)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (13)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsNo ratings yet
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (3)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (4)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (32)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (41)
- The Tennis Partner: A Doctor's Story of Friendship and LossFrom EverandThe Tennis Partner: A Doctor's Story of Friendship and LossRating: 4.5 out of 5 stars4.5/5 (4)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)