You might also like
- Pharmacology Notes #1 DRUG ACTIONDocument4 pagesPharmacology Notes #1 DRUG ACTIONAyumi StarNo ratings yet
- Anatomy and Physiology of The StomachDocument7 pagesAnatomy and Physiology of The StomachEmmi Maliza HutagaolNo ratings yet
- Pharmacology Notes Chapter 1 IntroDocument4 pagesPharmacology Notes Chapter 1 Introridley45No ratings yet
- Anatomy and Physiology of BloodDocument10 pagesAnatomy and Physiology of Bloodaoi_rachelle100% (1)
- Biochem Laboratory Activity 2Document4 pagesBiochem Laboratory Activity 2Kristine PangahinNo ratings yet
- Stool Analysis (D/R) TestDocument8 pagesStool Analysis (D/R) TestAbed AbusalemNo ratings yet
- Demonstration of The Reflex Pathway in FrogsDocument12 pagesDemonstration of The Reflex Pathway in FrogsRuwiniRajakarunaNo ratings yet
- AntibioticsDocument22 pagesAntibioticsEllen Castillo MarianoNo ratings yet
- Respiratory SystemDocument89 pagesRespiratory SystemSuzuke Mae Nijo100% (1)
- CC1 Lab Fin V2Document22 pagesCC1 Lab Fin V2Melody PardilloNo ratings yet
- AntidoteDocument5 pagesAntidoteMaynard ArandaNo ratings yet
- DIGESTIVE SYSTEM BREAKDOWNDocument7 pagesDIGESTIVE SYSTEM BREAKDOWNtheodore_estradaNo ratings yet
- Kidney Nephron Structure and FunctionDocument4 pagesKidney Nephron Structure and Functionxanxan4321No ratings yet
- Common Parasitic Infections - Life Cycles and TreatmentsDocument7 pagesCommon Parasitic Infections - Life Cycles and TreatmentsAj MillanNo ratings yet
- Anatomy and Physiology With Pathophysiology TransesDocument10 pagesAnatomy and Physiology With Pathophysiology Transeshezekiah minNo ratings yet
- Anatomy and physiology of bloodDocument4 pagesAnatomy and physiology of bloodDylle Lorenzo ClaudioNo ratings yet
- Renal Anatomy & Physiology OverviewDocument5 pagesRenal Anatomy & Physiology OverviewChristopher BucuNo ratings yet
- Gram StainDocument5 pagesGram Stainادم PrabowoNo ratings yet
- 35 Drugs Used DyslipidemiaDocument58 pages35 Drugs Used DyslipidemiaNibshian Dela RosaNo ratings yet
- Serum ElectrolytesDocument2 pagesSerum ElectrolytesKervin CablaidaNo ratings yet
- Transfusion TherapyDocument29 pagesTransfusion Therapyoxidalaj100% (3)
- Heparin: A Highly Sulfated Glycosaminoglycan Used as an AnticoagulantDocument14 pagesHeparin: A Highly Sulfated Glycosaminoglycan Used as an Anticoagulantanirbanmanna88320100% (1)
- Hiv & Aids-Related Drugs: Pharma - Semis GutierrezDocument3 pagesHiv & Aids-Related Drugs: Pharma - Semis GutierrezYsabelle GutierrezNo ratings yet
- Hematology: - The Science Dealing With The FormationDocument104 pagesHematology: - The Science Dealing With The FormationYamSomandarNo ratings yet
- Fluids and ElectrolytesBlood TransfusionDocument6 pagesFluids and ElectrolytesBlood TransfusionMaria Erica Jan MirandaNo ratings yet
- (CLINPATH) Lipids and DyslipoproteinemiaDocument5 pages(CLINPATH) Lipids and DyslipoproteinemiaJolaine ValloNo ratings yet
- Pharmacology Notes #1Document2 pagesPharmacology Notes #1Ayumi StarNo ratings yet
- Practical 1-Far 161-FinishDocument10 pagesPractical 1-Far 161-FinishZulkifli Khairuddin100% (1)
- Genitourinary Tract InfectionsDocument80 pagesGenitourinary Tract Infectionsraene_bautistaNo ratings yet
- Pharmacology 1Document53 pagesPharmacology 1Dawn WRein LegaspiNo ratings yet
- Fluid Electrolyte Acid-Base BalanceDocument17 pagesFluid Electrolyte Acid-Base BalanceBethany HoffmanNo ratings yet
- Chap 14 Micropara ReviewerDocument25 pagesChap 14 Micropara RevieweryanNo ratings yet
- Biochemistry JD 2Document6 pagesBiochemistry JD 2failinNo ratings yet
- Microbiology-Specimens CollectionDocument31 pagesMicrobiology-Specimens Collectionapi-253201876100% (1)
- Compilation Medsurg PrelimsDocument29 pagesCompilation Medsurg PrelimsEunice CuñadaNo ratings yet
- FLUIDS AND ELECTROLYTES: MAINTAINING BALANCEDocument13 pagesFLUIDS AND ELECTROLYTES: MAINTAINING BALANCEhahahahaaaaaaa100% (1)
- PL1 3Document2 pagesPL1 3Dennis Valdez80% (5)
- Urinary System and Disorders IntroductionDocument23 pagesUrinary System and Disorders IntroductionHananya ManroeNo ratings yet
- Oral Drug Absorption Factors and ClassificationDocument11 pagesOral Drug Absorption Factors and ClassificationClarilaine JavierNo ratings yet
- Pancreatic Enzymes Help Digest CarbsDocument7 pagesPancreatic Enzymes Help Digest CarbsAngelaAmmcoNo ratings yet
- 10mm Frog Lungbud-AnusDocument11 pages10mm Frog Lungbud-Anusaa628100% (2)
- OsmometryDocument6 pagesOsmometryVERMADEEN0% (1)
- Gastrointestinal Tract System NotesDocument8 pagesGastrointestinal Tract System NotesCarl Elexer Cuyugan Ano100% (1)
- Different Types of VaccinesDocument4 pagesDifferent Types of VaccinesTenisha KnowlesNo ratings yet
- Semen Analysis (Seminal Cytology, Sperm CountDocument30 pagesSemen Analysis (Seminal Cytology, Sperm Countabdurae100% (1)
- PMLS FinalsDocument20 pagesPMLS FinalsPhilipp LibasoraNo ratings yet
- Biochemistry Week 3 - EnzymesDocument6 pagesBiochemistry Week 3 - EnzymesMicah JadeNo ratings yet
- TrematodesDocument9 pagesTrematodesLewis P. SanchezNo ratings yet
- Hematology 2 TEST QUESTIONSDocument4 pagesHematology 2 TEST QUESTIONSa a r o n b a u t i s t aNo ratings yet
- The HIV Life CycleDocument1 pageThe HIV Life Cycleapi-3732057100% (1)
- RBC CountsDocument16 pagesRBC Countsalmastar officeNo ratings yet
- Sporozoa 4Document27 pagesSporozoa 4ebenezermanzanormtNo ratings yet
- MLS312 - Module04 - Explore - Experiment#6 - 0962 - Calpahi - Justine JadeDocument4 pagesMLS312 - Module04 - Explore - Experiment#6 - 0962 - Calpahi - Justine JadeJustine Jade Atew CalpahiNo ratings yet
- The Intestinal NematodesDocument9 pagesThe Intestinal NematodesdhaineyNo ratings yet
- Direct Fecal Smear (Saline and Iodine Wet Mount Preparations)Document6 pagesDirect Fecal Smear (Saline and Iodine Wet Mount Preparations)Tom Anthony TonguiaNo ratings yet
- 1.introduction To PharmacologyDocument127 pages1.introduction To PharmacologyblacknurseNo ratings yet
- Pharmacologic PrinciplesDocument57 pagesPharmacologic PrinciplesYousef Jafar100% (1)
- NCM 106 Drugs and The BodyDocument46 pagesNCM 106 Drugs and The BodyYra JhaneNo ratings yet
- Pharmacology Transes - Unit 1Document13 pagesPharmacology Transes - Unit 1venturaphoenixNo ratings yet
- 3 Principles of Drug Actions and InteractionsDocument6 pages3 Principles of Drug Actions and InteractionsBernardMarkMateoNo ratings yet
- JNC 8Document2 pagesJNC 8ririnrahayumsNo ratings yet
- JNC 8 Guideline Algorithm for Treating HypertensionDocument2 pagesJNC 8 Guideline Algorithm for Treating HypertensionTaradifaNurInsi0% (1)
- CPG GoutDocument2 pagesCPG GoutRomie SolacitoNo ratings yet
- Philippine Clinical Practice Guidelines For The Management of Gout 2008Document7 pagesPhilippine Clinical Practice Guidelines For The Management of Gout 2008JedNo ratings yet
- Antistreptolysin oDocument13 pagesAntistreptolysin oRomie SolacitoNo ratings yet
- Clinical Chemistry: ChlorideDocument2 pagesClinical Chemistry: ChlorideRomie SolacitoNo ratings yet
- Electrolytes PDFDocument8 pagesElectrolytes PDFRomie SolacitoNo ratings yet
- JSC 130010Document14 pagesJSC 130010drprissaNo ratings yet
- Philippine Clinical Practice Guidelines On The Medical Management of Osteoarthritis of The KneeDocument15 pagesPhilippine Clinical Practice Guidelines On The Medical Management of Osteoarthritis of The KneeJames JavierNo ratings yet
- Clinical Chemistry: PotassiumDocument4 pagesClinical Chemistry: PotassiumRomie SolacitoNo ratings yet
- ISBB - Week 3Document8 pagesISBB - Week 3Romie SolacitoNo ratings yet
- Thyroid GlandDocument54 pagesThyroid GlandRomie SolacitoNo ratings yet
- Clinical Chemistry: CalciumDocument5 pagesClinical Chemistry: CalciumRomie SolacitoNo ratings yet
- ISBBDocument26 pagesISBBRomie SolacitoNo ratings yet
- Urine CrystalsDocument4 pagesUrine CrystalsRomie SolacitoNo ratings yet
- Introduction To ParasitologyDocument2 pagesIntroduction To ParasitologyRomie SolacitoNo ratings yet
- Copper Deficiency Anemia and Neutropenia Due To Ketogenic DietDocument11 pagesCopper Deficiency Anemia and Neutropenia Due To Ketogenic DietRomie SolacitoNo ratings yet
- Clinical Hematology Case StudyDocument6 pagesClinical Hematology Case StudyRomie SolacitoNo ratings yet
- Hematoxylin and Eosin ProcedureDocument1 pageHematoxylin and Eosin ProcedureRomie SolacitoNo ratings yet
- Microbiology Case Study: Cryptococcal MeningitisDocument16 pagesMicrobiology Case Study: Cryptococcal MeningitisRomie SolacitoNo ratings yet
- Immuno-Serology & Blood Banking Case Study: Systemic Lupus ErythematosusDocument6 pagesImmuno-Serology & Blood Banking Case Study: Systemic Lupus ErythematosusRomie SolacitoNo ratings yet
- Immuno-Serology & Blood Banking Case StudyDocument8 pagesImmuno-Serology & Blood Banking Case StudyRomie SolacitoNo ratings yet
- Yeast Invasion of Male's Central Nervous SystemDocument9 pagesYeast Invasion of Male's Central Nervous SystemRomie SolacitoNo ratings yet
- Immuno-Serology: Antistreptolysin 0Document13 pagesImmuno-Serology: Antistreptolysin 0Romie SolacitoNo ratings yet
- UIC Medical Laboratory Science Preliminary Defense on Anti-Streptolysin O TestDocument1 pageUIC Medical Laboratory Science Preliminary Defense on Anti-Streptolysin O TestRomie SolacitoNo ratings yet
- DNA to Cells: A Brief History of CytogeneticsDocument5 pagesDNA to Cells: A Brief History of CytogeneticsRomie SolacitoNo ratings yet
- MICROSCOPIC EXAMINATION OF URINE SEDIMENTDocument14 pagesMICROSCOPIC EXAMINATION OF URINE SEDIMENTRomie Solacito100% (1)
- AUBF - PreliminariesDocument5 pagesAUBF - PreliminariesRomie SolacitoNo ratings yet
- Immunology & Serology: Preliminaries: Romie Solacito, MLS3CDocument12 pagesImmunology & Serology: Preliminaries: Romie Solacito, MLS3CRomie Solacito100% (2)
- Manual Videoporteiro Tuya Painel de Chamada 84218Document6 pagesManual Videoporteiro Tuya Painel de Chamada 84218JGC CoimbraNo ratings yet
- P. L. MacKendrick - Roman ColonizationDocument9 pagesP. L. MacKendrick - Roman ColonizationAnyád ApádNo ratings yet
- Lessons From Nothing - Activities For Language Teaching With Limited Time and Resources (Cambridge Handbooks For Language Teachers) 2Document121 pagesLessons From Nothing - Activities For Language Teaching With Limited Time and Resources (Cambridge Handbooks For Language Teachers) 2Ryan Ryan100% (1)
- Electric Expansion Valve: Type ETS 12.5 - ETS 400Document18 pagesElectric Expansion Valve: Type ETS 12.5 - ETS 400Mustafa MouradNo ratings yet
- Housing Typologies & Development in The PhilippinesDocument5 pagesHousing Typologies & Development in The Philippinesmaria lourdes bautista100% (1)
- Importance of Bus Rapid Transit Systems (BRTSDocument7 pagesImportance of Bus Rapid Transit Systems (BRTSAnshuman SharmaNo ratings yet
- Lineas de Inyeccion 320c MaaDocument3 pagesLineas de Inyeccion 320c MaaHAmir Alberto Mojica MojicaNo ratings yet
- DIY Mini CNC Laser EngraverDocument194 pagesDIY Mini CNC Laser EngraverPier DanNo ratings yet
- Zoomorphology: Morphology and Function of The Tube Feet of (Echinodermata: Crinoidea)Document13 pagesZoomorphology: Morphology and Function of The Tube Feet of (Echinodermata: Crinoidea)Indra SatriaNo ratings yet
- Analyze The NatureDocument2 pagesAnalyze The Naturewaril30558No ratings yet
- Lesson Plans: Pre A1 Starters Reading & Writing Part 2 - Teacher's NotesDocument5 pagesLesson Plans: Pre A1 Starters Reading & Writing Part 2 - Teacher's NotesRon ChowdhuryNo ratings yet
- User's Manual: & Technical DocumentationDocument20 pagesUser's Manual: & Technical DocumentationPODOSALUD HUANCAYONo ratings yet
- Autism and Autism Spectrum Disorder Medical Hypothesis For Parasites Influencing AutismDocument3 pagesAutism and Autism Spectrum Disorder Medical Hypothesis For Parasites Influencing AutismCATHYNo ratings yet
- Guidelines For Writing MSC Synopsis or Research ProposalDocument24 pagesGuidelines For Writing MSC Synopsis or Research ProposalFahd100% (1)
- Relative ClausesDocument7 pagesRelative ClausesEvaluna MoidalNo ratings yet
- ConcreteDocument1 pageConcreteRyan_RajmoolieNo ratings yet
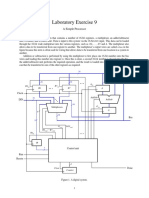
- Laboratory Exercise 9: A Simple ProcessorDocument8 pagesLaboratory Exercise 9: A Simple ProcessorhxchNo ratings yet
- A Formalist Approach To Robert FrostDocument6 pagesA Formalist Approach To Robert FrostAdel75% (4)
- Strategies of Literary TranslationDocument7 pagesStrategies of Literary TranslationMuhammad J H AbdullatiefNo ratings yet
- KA7630/KA7631: Fixed Multi-Output RegulatorDocument6 pagesKA7630/KA7631: Fixed Multi-Output RegulatorTecnico GenioNo ratings yet
- The Role of NNN in Zeolite Acidity and ActivityDocument25 pagesThe Role of NNN in Zeolite Acidity and ActivityRaj MehtaNo ratings yet
- IES VE Parametric Tool GuideDocument7 pagesIES VE Parametric Tool GuideDaisy ForstnerNo ratings yet
- Gartner - Predicts 2021 - Accelerate - Results - Beyond - RPA - To - Hyperautomation-2020Q4Document17 pagesGartner - Predicts 2021 - Accelerate - Results - Beyond - RPA - To - Hyperautomation-2020Q4Guille LopezNo ratings yet
- Class Discussion QuestionsDocument2 pagesClass Discussion Questionshank hillNo ratings yet
- Kyrin Trapp 1st Grade Language Arts Lesson PlanDocument4 pagesKyrin Trapp 1st Grade Language Arts Lesson PlanKyrin TrappNo ratings yet
- 3I'S (Week 7-8)Document15 pages3I'S (Week 7-8)AldrinJosephLacuarinNo ratings yet
- Antacid Booklet Final Sept 2015Document49 pagesAntacid Booklet Final Sept 2015MarianelaMolocheNo ratings yet
- HP Police Constable Question Paper 2015Document9 pagesHP Police Constable Question Paper 2015Rajat SharmãNo ratings yet
- Assignment IDocument4 pagesAssignment IDylan HsiehNo ratings yet
- 9.36 Project Summary FormDocument2 pages9.36 Project Summary FormTu Burin DtNo ratings yet