You might also like
- Critical Appraisal for Therapy ArticlesDocument4 pagesCritical Appraisal for Therapy ArticlesMahardhika AcintyaNo ratings yet
- Critical Appraisal TafaDocument7 pagesCritical Appraisal TafaFabric FameNo ratings yet
- Critical ApraisalDocument4 pagesCritical Apraisalfauziah qurrota a'yuniNo ratings yet
- Referat Iktiosis PembahasanDocument4 pagesReferat Iktiosis PembahasanPatih GajahmadaNo ratings yet
- Worksheet Appraisal AZALEADocument5 pagesWorksheet Appraisal AZALEAArini NurlelaNo ratings yet
- Centralised Computer Randomisation Is: Critical Appraisal For Therapy ArticlesDocument4 pagesCentralised Computer Randomisation Is: Critical Appraisal For Therapy ArticleshadzaliegNo ratings yet
- Patients - Intervention - Comparison - Outcome(s) - Knowledge GapDocument4 pagesPatients - Intervention - Comparison - Outcome(s) - Knowledge GapAmal NajiNo ratings yet
- Critical Appraisal Jurnal India WiwinDocument6 pagesCritical Appraisal Jurnal India WiwinWindy Atika HapsariNo ratings yet
- THERAPY STUDY RESULTS VALIDDocument4 pagesTHERAPY STUDY RESULTS VALIDAhmad BukhariNo ratings yet
- RCT Appraisal Sheets 2005 English-1 1Document5 pagesRCT Appraisal Sheets 2005 English-1 1api-479716004No ratings yet
- Therapy Studies What Question Did The Study Ask?Document2 pagesTherapy Studies What Question Did The Study Ask?Apt RiskaNo ratings yet
- RCT Appraisal Sheets 2005 English-2Document6 pagesRCT Appraisal Sheets 2005 English-2tsyrahmaniNo ratings yet
- Kritisi Artikel - Ni Nengah Susilawati - 152191105 - BDocument5 pagesKritisi Artikel - Ni Nengah Susilawati - 152191105 - BShilaNo ratings yet
- (OBAT CINA) CAT TherapyDocument6 pages(OBAT CINA) CAT TherapyArga PRNo ratings yet
- RCT Appraisal Sheets 2005 EnglishDocument4 pagesRCT Appraisal Sheets 2005 EnglishAmanda SoebadiNo ratings yet
- Therapystudy: Are The Results of The Trial Valid? (Internal Validity)Document6 pagesTherapystudy: Are The Results of The Trial Valid? (Internal Validity)Sinta AgustinaNo ratings yet
- Worksheet Therapy CebmDocument3 pagesWorksheet Therapy Cebmandynightmare97No ratings yet
- Critical Appraisal For Therapy Articles: Are The Results of The Trial Valid? (Internal Validity)Document4 pagesCritical Appraisal For Therapy Articles: Are The Results of The Trial Valid? (Internal Validity)Putri Widya AndiniNo ratings yet
- Therapystudy: Are The Results of The Trial Valid? (Internal Validity)Document10 pagesTherapystudy: Are The Results of The Trial Valid? (Internal Validity)WiraNo ratings yet
- RCT Appraisal Sheets 2005 EnglishDocument2 pagesRCT Appraisal Sheets 2005 EnglishF NNo ratings yet
- Patients - Intervention - Comparison - Outcome(s)Document3 pagesPatients - Intervention - Comparison - Outcome(s)Intan SetyadewiNo ratings yet
- Tugas Farepid - CA - 198114152Document11 pagesTugas Farepid - CA - 198114152JeanieNo ratings yet
- C - II - 3 - Critical AppraisalDocument10 pagesC - II - 3 - Critical AppraisalWahyu NandaNo ratings yet
- Worksheet Therapy-CebmDocument3 pagesWorksheet Therapy-Cebmteddy sNo ratings yet
- Critical Therapy Study ResultsDocument4 pagesCritical Therapy Study ResultsAinur 'iin' RahmahNo ratings yet
- Patients - Intervention - Comparison - Outcome(s)Document4 pagesPatients - Intervention - Comparison - Outcome(s)sahirbuleNo ratings yet
- Critical Appraisal Jurnal Asam Traneksamat Pada MelasmaDocument4 pagesCritical Appraisal Jurnal Asam Traneksamat Pada MelasmaMsrirrrNo ratings yet
- Checklist RCTDocument5 pagesChecklist RCTFajar SukmajayaNo ratings yet
- EBM Dan Critical AppraisalDocument7 pagesEBM Dan Critical AppraisalNovia Ariani DewiNo ratings yet
- CRITICAL APPRAISAL Mas WikoDocument10 pagesCRITICAL APPRAISAL Mas WikoEliataMariaMahanaimNo ratings yet
- Randomised: Differences Between Groups Are Statistically Significant P ValuesDocument6 pagesRandomised: Differences Between Groups Are Statistically Significant P ValuesArga PRNo ratings yet
- CA Therapy Artikel 09Document5 pagesCA Therapy Artikel 09Christiana TrijayantiNo ratings yet
- Anesthesiologists (ASA) I: THERAPY STUDY: Are The Results of The Trial Valid? (Internal Validity)Document4 pagesAnesthesiologists (ASA) I: THERAPY STUDY: Are The Results of The Trial Valid? (Internal Validity)Sandra Lydiayana Aisyah AzharNo ratings yet
- Critical Appraisal Checklist For An Article OnDocument4 pagesCritical Appraisal Checklist For An Article OnTiaz DiniutamiNo ratings yet
- Critical Appraisal for Therapy Study ResultsDocument3 pagesCritical Appraisal for Therapy Study ResultsVeysusanNo ratings yet
- Critical Appraisal of Therapy Study ValidityDocument3 pagesCritical Appraisal of Therapy Study ValidityOtty Mitha OctrizaNo ratings yet
- DPS: Evidence Based Medicine and Clinical Epidemiology: Types of Research QuestionDocument37 pagesDPS: Evidence Based Medicine and Clinical Epidemiology: Types of Research Questionarjun.k5796No ratings yet
- Critical Appraisal Checklist For An Article On Treatment or PreventionDocument4 pagesCritical Appraisal Checklist For An Article On Treatment or PreventionSaina AbasNo ratings yet
- Twice Weekly FluticasoneDocument4 pagesTwice Weekly FluticasoneAudrey GillNo ratings yet
- Critical Appraisal for Therapy Studies WorksheetDocument2 pagesCritical Appraisal for Therapy Studies WorksheetAdwin AlamsyaputraNo ratings yet
- Critical Appraisal For RCT & Meta AnalisisDocument8 pagesCritical Appraisal For RCT & Meta AnalisisHanniNo ratings yet
- Laporan Resmi Praktikum Pharmaceutical Kardio Endokrin Pertemuan V Critical Appraisal (Ebm)Document16 pagesLaporan Resmi Praktikum Pharmaceutical Kardio Endokrin Pertemuan V Critical Appraisal (Ebm)evangeline keisha annabelNo ratings yet
- Telaah Kritis Jurnal 2Document9 pagesTelaah Kritis Jurnal 2Ayu Vitha ViginiaNo ratings yet
- Crit AppDocument5 pagesCrit AppdikkaNo ratings yet
- Make A NewSenin 26 Januari 2015 EBM GLOSARY Dr. Akhmad EdiDocument12 pagesMake A NewSenin 26 Januari 2015 EBM GLOSARY Dr. Akhmad EdinaotonaoiNo ratings yet
- Evidence-Based Medicine Therapy: Dr. Dr. Rina Amelia, MARS Departemen Kedokteran Komunitas FK USUDocument40 pagesEvidence-Based Medicine Therapy: Dr. Dr. Rina Amelia, MARS Departemen Kedokteran Komunitas FK USUSamuel TanNo ratings yet
- Critical Appraisal EBM-Therapy Journal IDocument29 pagesCritical Appraisal EBM-Therapy Journal IJosephine IrenaNo ratings yet
- "Evidence-Based Medicine" TherapyDocument54 pages"Evidence-Based Medicine" TherapyRuthra Devi NarayanasamyNo ratings yet
- WS-terapy-Frisbe-contoh-DVT 3Document3 pagesWS-terapy-Frisbe-contoh-DVT 3Ina RahmaNo ratings yet
- Minor Stroke Recovery Study Compares DrugsDocument14 pagesMinor Stroke Recovery Study Compares Drugsevangeline keisha annabelNo ratings yet
- Evidence-Based Medicine Therapy: Dr. Rina Amelia, MARSDocument43 pagesEvidence-Based Medicine Therapy: Dr. Rina Amelia, MARSRezky IlhamNo ratings yet
- Presentation On TherapyDocument21 pagesPresentation On TherapyMarjorie CepeNo ratings yet
- Critical Appraisal JRDocument3 pagesCritical Appraisal JRRizky AgustriaNo ratings yet
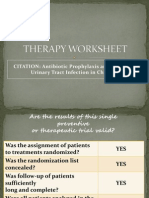
- CITATION: Antibiotic Prophylaxis and Recurrent Urinary Tract Infection in ChildrenDocument16 pagesCITATION: Antibiotic Prophylaxis and Recurrent Urinary Tract Infection in Childrenchristian_friztNo ratings yet
- Measurement of Out CDocument62 pagesMeasurement of Out CrafaidaabubakarNo ratings yet
- Prognosis Question Critical AppraisalDocument2 pagesPrognosis Question Critical AppraisalLee ARyNo ratings yet
- EBM Probiotics For BacvagDocument12 pagesEBM Probiotics For BacvagJeanne Mae Lee AfallaNo ratings yet
- Cat 2Document5 pagesCat 2marieclairemarty19No ratings yet
- Supportive Care in Pediatric Oncology: A Practical Evidence-Based ApproachFrom EverandSupportive Care in Pediatric Oncology: A Practical Evidence-Based ApproachJames H. FeusnerNo ratings yet
- Anti-Aging Therapeutics Volume XIIIFrom EverandAnti-Aging Therapeutics Volume XIIINo ratings yet
- Journal of Epidemiology and Global HealthDocument7 pagesJournal of Epidemiology and Global HealthZulfan RifqiawanNo ratings yet
- M2 Hookworms (Apik)Document4 pagesM2 Hookworms (Apik)Zulfan RifqiawanNo ratings yet
- Pemeriksaan Laboratorium Hormon Tiroid: Oleh: Dr. Diah Hermayanti, SPPKDocument16 pagesPemeriksaan Laboratorium Hormon Tiroid: Oleh: Dr. Diah Hermayanti, SPPKZulfan RifqiawanNo ratings yet
- Overview of The CDC Growth Charts: CDC: Safer - Healthier - People 1Document25 pagesOverview of The CDC Growth Charts: CDC: Safer - Healthier - People 1Batako HayashiNo ratings yet
- Three Clinical Cases of Cutaneus Larva MigransDocument6 pagesThree Clinical Cases of Cutaneus Larva MigransAndre FernandesNo ratings yet
- Cutaneous Larva Migrans DynaMed (Prevalence)Document9 pagesCutaneous Larva Migrans DynaMed (Prevalence)Zulfan RifqiawanNo ratings yet
- Case Report Abortus Spontan IncompleteDocument6 pagesCase Report Abortus Spontan IncompleteIola SalsabilaNo ratings yet
- Hookworms AkramDocument21 pagesHookworms AkramZulfan RifqiawanNo ratings yet
- 72 223 1 PBDocument12 pages72 223 1 PBKatarina fransiscaNo ratings yet
- Materi Kuliah OrtopediDocument6 pagesMateri Kuliah OrtopediZulfan RifqiawanNo ratings yet
- Hookworms MTN View 1Document5 pagesHookworms MTN View 1Zulfan RifqiawanNo ratings yet
- The Hookworm Ancylostoma Ceylanicum: An Emerging Public Health Risk in Australian Tropical Rainforests And..Document5 pagesThe Hookworm Ancylostoma Ceylanicum: An Emerging Public Health Risk in Australian Tropical Rainforests And..Zulfan RifqiawanNo ratings yet
- Data Base Clue and CUE Problem List Initial Diagnosis Planning Diagnosis Therapy Monitoring EducationDocument2 pagesData Base Clue and CUE Problem List Initial Diagnosis Planning Diagnosis Therapy Monitoring EducationnadiadhilaNo ratings yet
- Materi Kuliah OrtopediDocument6 pagesMateri Kuliah OrtopediZulfan RifqiawanNo ratings yet
- Data Base Clue and CUE Problem List Initial Diagnosis Planning Diagnosis Therapy Monitoring EducationDocument2 pagesData Base Clue and CUE Problem List Initial Diagnosis Planning Diagnosis Therapy Monitoring EducationnadiadhilaNo ratings yet
- Cutaneous Creeping Eruption in A Child: Shrikiran Aroor, Sandeep Kumar, Suneel MundkurDocument2 pagesCutaneous Creeping Eruption in A Child: Shrikiran Aroor, Sandeep Kumar, Suneel MundkurZulfan RifqiawanNo ratings yet
- Heuk El Bach 2008Document8 pagesHeuk El Bach 2008Zulfan RifqiawanNo ratings yet
- Cutaneous Creeping Eruption in A Child: Shrikiran Aroor, Sandeep Kumar, Suneel MundkurDocument2 pagesCutaneous Creeping Eruption in A Child: Shrikiran Aroor, Sandeep Kumar, Suneel MundkurZulfan RifqiawanNo ratings yet
- Hookworms 鉤蟲: Distribution betweenDocument14 pagesHookworms 鉤蟲: Distribution betweenZulfan RifqiawanNo ratings yet
- Ancylostoma ceylanicum Hookworm Species Found Endemic in Solomon IslandsDocument7 pagesAncylostoma ceylanicum Hookworm Species Found Endemic in Solomon IslandsZulfan RifqiawanNo ratings yet
- Daftar Pustaka Pualing BaruDocument4 pagesDaftar Pustaka Pualing BaruZulfan RifqiawanNo ratings yet
- Issue in Html2016!1!34Document20 pagesIssue in Html2016!1!34Zulfan RifqiawanNo ratings yet
- Ancylostoma ceylanicum Hookworm Species Found Endemic in Solomon IslandsDocument7 pagesAncylostoma ceylanicum Hookworm Species Found Endemic in Solomon IslandsZulfan RifqiawanNo ratings yet
- Validity and ReliabilityDocument19 pagesValidity and ReliabilityZulfan Rifqiawan100% (4)
- FeverDocument0 pagesFeverRegina SeptianiNo ratings yet
- Judul Pengaruh Pemberian Seduhan Kulit Jambu Air (Syzygium Maleccense) Terhadap Penurunan Kolesterol Total Pada Tikus PutihDocument1 pageJudul Pengaruh Pemberian Seduhan Kulit Jambu Air (Syzygium Maleccense) Terhadap Penurunan Kolesterol Total Pada Tikus PutihZulfan RifqiawanNo ratings yet
- 10 1088@1757-899X@193@1@012057 PDFDocument7 pages10 1088@1757-899X@193@1@012057 PDFZulfan RifqiawanNo ratings yet
- Prevalence of Hookworm Infection Among Patients Attending Aminu Kano Teaching Hospital Kano, NigeriaDocument3 pagesPrevalence of Hookworm Infection Among Patients Attending Aminu Kano Teaching Hospital Kano, NigeriaZulfan RifqiawanNo ratings yet
- 10 1088@1757-899X@193@1@012057 PDFDocument7 pages10 1088@1757-899X@193@1@012057 PDFZulfan RifqiawanNo ratings yet
- Indian Disinfectant Industry LeadersDocument4 pagesIndian Disinfectant Industry LeadersSanjukt K. SahaNo ratings yet
- Name: - Date: - SectionDocument5 pagesName: - Date: - SectionJunjun CaoliNo ratings yet
- Intake and Output (I and O) Monitoring Brief DescriptionDocument4 pagesIntake and Output (I and O) Monitoring Brief DescriptionJan Crizza Dale R. FrancoNo ratings yet
- CURRENT STATUS OF CHILD HEALTH IN INDIA To Be PrintDocument6 pagesCURRENT STATUS OF CHILD HEALTH IN INDIA To Be Printprecillathoppil96% (24)
- Accomplishment Report 2020Document6 pagesAccomplishment Report 2020Jaileen BatiancilaNo ratings yet
- Essay 2Document4 pagesEssay 2api-508702818No ratings yet
- Inservice PresentationDocument13 pagesInservice Presentationapi-467829418No ratings yet
- Helping Patients With Paranoid and Suspicious Thoughts A Cognitivebehavioural ApproachDocument12 pagesHelping Patients With Paranoid and Suspicious Thoughts A Cognitivebehavioural ApproachNunoNo ratings yet
- Comunicaciœn No VerbalDocument13 pagesComunicaciœn No VerbalRosangelina A. MartinezNo ratings yet
- Hospital Dietary Services Planning and ManagementDocument12 pagesHospital Dietary Services Planning and ManagementAnkit TalujaNo ratings yet
- CHD With NCPDocument10 pagesCHD With NCPJohanna Kirsten F. DaguioNo ratings yet
- Emergency Preparedness and ResponseDocument32 pagesEmergency Preparedness and ResponseMd Rokib ChowdhuryNo ratings yet
- High School DropoutDocument7 pagesHigh School Dropoutapi-318407875No ratings yet
- DiphtheriaDocument4 pagesDiphtheriaRickiko HardiNo ratings yet
- Medscape All Covid 19Document81 pagesMedscape All Covid 19david dompeipenNo ratings yet
- Diabetes Foot Care Education Resource Pack: June 2016Document16 pagesDiabetes Foot Care Education Resource Pack: June 2016AthenaNo ratings yet
- Renal Tumor and Polycystic Kidney DiseaseDocument6 pagesRenal Tumor and Polycystic Kidney DiseaseMahdawwNo ratings yet
- n597 Psychiatric EvalDocument11 pagesn597 Psychiatric Evalapi-532870494No ratings yet
- Covid Patients2022Document221 pagesCovid Patients2022Sample BakeshopNo ratings yet
- Sepulveda 2002 Paliative Care Who PerspectiveDocument6 pagesSepulveda 2002 Paliative Care Who PerspectiveDaniela MunteleNo ratings yet
- Belizario VicenteDocument15 pagesBelizario VicenteRoshanDavidNo ratings yet
- Clinical Paperwork 2014-2015Document8 pagesClinical Paperwork 2014-2015AmandaNicholsNo ratings yet
- First Aid Skill Retention of First Responders Within The WorkplaceDocument6 pagesFirst Aid Skill Retention of First Responders Within The WorkplaceYusri RamliNo ratings yet
- Yoga Final Assignment Pigeon PoseDocument4 pagesYoga Final Assignment Pigeon Poseapi-341211173No ratings yet
- Fentanyl Dosage and Nursing ResponsibilitiesDocument3 pagesFentanyl Dosage and Nursing ResponsibilitiesDavid Villanueva67% (3)
- BDP - Brgy. AcunaDocument37 pagesBDP - Brgy. AcunaMarnieNo ratings yet
- Weekly Influenza Report WeekDocument9 pagesWeekly Influenza Report WeekKATVNo ratings yet
- Health Declaration FormDocument2 pagesHealth Declaration FormMark Israel DirectoNo ratings yet
- SW 3020 Biopsychosocial Paper 1-Anika-LaptopDocument19 pagesSW 3020 Biopsychosocial Paper 1-Anika-Laptopapi-282542988100% (1)
- Clinical Practice Guidelines For Antimicrobial Prophylaxis in Surgery (Update 2013)Document89 pagesClinical Practice Guidelines For Antimicrobial Prophylaxis in Surgery (Update 2013)เด็กชายสมันตภัทร แฟนคลับอาจารย์กวงNo ratings yet