You might also like
- Disorders of The Oral CavityDocument60 pagesDisorders of The Oral CavityDenesha KaurNo ratings yet
- Febrile Fit: Foong Wei Jian Denesha KaurDocument19 pagesFebrile Fit: Foong Wei Jian Denesha KaurDenesha KaurNo ratings yet
- Febrile Fit: Foong Wei Jian Denesha KaurDocument19 pagesFebrile Fit: Foong Wei Jian Denesha KaurDenesha KaurNo ratings yet
- Five Rights of Drug Admin PowerpointDocument32 pagesFive Rights of Drug Admin Powerpointterobau123No ratings yet
- Pharmacology TerminologiesDocument8 pagesPharmacology TerminologiesDenesha Kaur100% (1)
- FractionsDocument4 pagesFractionsDenesha KaurNo ratings yet
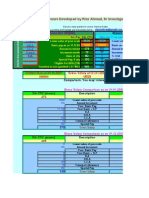
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- MNB - Code of Prof ConductDocument4 pagesMNB - Code of Prof ConductArisya Noor AhmadNo ratings yet
- BiochemistryDocument35 pagesBiochemistryDenesha KaurNo ratings yet
- Pharmacologic Principles: - Additive EffectsDocument8 pagesPharmacologic Principles: - Additive EffectsDenesha KaurNo ratings yet
- Pharmacologic Principles: - Additive EffectsDocument8 pagesPharmacologic Principles: - Additive EffectsDenesha KaurNo ratings yet
- Pharmacologic Principles: - Additive EffectsDocument8 pagesPharmacologic Principles: - Additive EffectsDenesha KaurNo ratings yet
- C2.3 How MuchDocument10 pagesC2.3 How MuchDenesha KaurNo ratings yet
- Year 10 Moles Calculations Homework 3Document1 pageYear 10 Moles Calculations Homework 3Denesha KaurNo ratings yet
- 3010 Adrenal and Parathyroid HormonesDocument21 pages3010 Adrenal and Parathyroid HormonesDenesha KaurNo ratings yet
- C2.1 Structures and BondingDocument6 pagesC2.1 Structures and BondingDenesha KaurNo ratings yet
- C7 Revision Earth and AtmosphereDocument2 pagesC7 Revision Earth and AtmosphereDenesha KaurNo ratings yet
- Chemistry: C4 Revision: Atomic StructureDocument1 pageChemistry: C4 Revision: Atomic StructureDenesha KaurNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Caesarean SectionDocument20 pagesCaesarean Sectionapi-3705046100% (3)
- Journal of Ethnopharmacology: Shashank Tiwari, Sandeep Kumar Gupta, Anklesh Kumar PathakDocument8 pagesJournal of Ethnopharmacology: Shashank Tiwari, Sandeep Kumar Gupta, Anklesh Kumar PathakMichael Kohlberger, BSc MScNo ratings yet
- ASD Overview: Causes, Symptoms, Diagnosis and TreatmentDocument22 pagesASD Overview: Causes, Symptoms, Diagnosis and TreatmentHendri SaputraNo ratings yet
- Medical Mnemonics 4 PrintDocument65 pagesMedical Mnemonics 4 Printanne0521100% (1)
- Effect of Intravenous Pamidronate Treatment in Children With Osteogenesis ImperfectaDocument5 pagesEffect of Intravenous Pamidronate Treatment in Children With Osteogenesis Imperfectavikash singhNo ratings yet
- FEVER & INFLUENZA INFORMATION FROM HARAPANAHALLI TALUK - Doctor Detail Patient DetailDocument3 pagesFEVER & INFLUENZA INFORMATION FROM HARAPANAHALLI TALUK - Doctor Detail Patient DetailaeepwdNo ratings yet
- BQ - Medical Writing Assignment-1Document1 pageBQ - Medical Writing Assignment-1Sumeet GurnaniNo ratings yet
- PHILAMCARE HEALTH SYSTEMS, INC., Petitioner, vs. COURT OF APPEALS and JULITA TRINOS, RespondentsDocument2 pagesPHILAMCARE HEALTH SYSTEMS, INC., Petitioner, vs. COURT OF APPEALS and JULITA TRINOS, RespondentsBert NazarioNo ratings yet
- Mechanical Ventilation Handout - AllenhoDocument23 pagesMechanical Ventilation Handout - AllenhoCarmen HerediaNo ratings yet
- COPD Case StudyDocument4 pagesCOPD Case StudyPj Declarador100% (4)
- Sepsis AlgorithmDocument1 pageSepsis AlgorithmAshly Nygil100% (1)
- COVID-19 Vaccination Certificate from India's Ministry of HealthDocument1 pageCOVID-19 Vaccination Certificate from India's Ministry of Healthbliss bNo ratings yet
- ArthropodaDocument36 pagesArthropodatapas kunduNo ratings yet
- Case AnaDocument12 pagesCase AnaBiel DelcanoNo ratings yet
- Understanding human factors in aviation safety and performanceDocument15 pagesUnderstanding human factors in aviation safety and performanceMoslem GrimaldiNo ratings yet
- Asepsis and Infection ControlDocument24 pagesAsepsis and Infection Controlabdisalaan hassanNo ratings yet
- q004 Little A Little Few A Few PDFDocument2 pagesq004 Little A Little Few A Few PDFmabel alicia marcial0% (1)
- Haemodynamic MonitoringDocument128 pagesHaemodynamic MonitoringDr. KNo ratings yet
- Practice Exam-10000 SeriesDocument12 pagesPractice Exam-10000 SeriesJuan Romero86% (28)
- Reparation, Characterization, and Optimization of Microemulsion For Topical Delivery of ItraconazoleDocument10 pagesReparation, Characterization, and Optimization of Microemulsion For Topical Delivery of ItraconazoleVeni UNNo ratings yet
- Lesson PlanDocument5 pagesLesson Planapi-456870847No ratings yet
- Laporan Praktikum Taksonomi Vertebrata RDocument10 pagesLaporan Praktikum Taksonomi Vertebrata RMuhammad Fahreza Rizky WNo ratings yet
- Chickpea: Vulgaris) and Dry Peas (Pisum Sativum L.) - Chickpea Seeds Contain On Average 18-22% ProteinDocument7 pagesChickpea: Vulgaris) and Dry Peas (Pisum Sativum L.) - Chickpea Seeds Contain On Average 18-22% ProteinGanpat Lal SharmaNo ratings yet
- Pad AbhyangaDocument7 pagesPad AbhyangaTrusha PatelNo ratings yet
- The Sense of Stopping Migraine ProphylaxisDocument20 pagesThe Sense of Stopping Migraine ProphylaxisdedeadamNo ratings yet
- Coping With Toxic Managers, Subordinates and Other Difficult PeopleDocument402 pagesCoping With Toxic Managers, Subordinates and Other Difficult Peoplejiggycheng91% (11)
- Task 46 Nina SharmanDocument3 pagesTask 46 Nina SharmanONT OETONLINENo ratings yet
- Warren 2009 RDSDocument13 pagesWarren 2009 RDSCIRUABCNo ratings yet
- Health Declaration Health Declaration: City of Mati City of MatiDocument2 pagesHealth Declaration Health Declaration: City of Mati City of MatiHannah Marie AlbeteNo ratings yet