You might also like
- Valeriano Prince RonnelDocument2 pagesValeriano Prince RonnelPRINCE RONNEL VALERIANONo ratings yet
- Health Assessment Form OriginalDocument3 pagesHealth Assessment Form Originaljd7vbm2tcqNo ratings yet
- Skills Checklist (HCA and Mental Health) - Copy (1710)Document2 pagesSkills Checklist (HCA and Mental Health) - Copy (1710)Mohammad Tayyab KhanNo ratings yet
- ED RN skills checklistDocument4 pagesED RN skills checklistJohn Carl Angelo EstrellaNo ratings yet
- Grade 12 Java Delos Santos Michael JacobDocument2 pagesGrade 12 Java Delos Santos Michael JacobJacob Delos SantosNo ratings yet
- Drug Mechanisms, Indications, Contraindications and Nursing ResponsibilitiesDocument5 pagesDrug Mechanisms, Indications, Contraindications and Nursing ResponsibilitiesNicko Pazon AranasNo ratings yet
- Patient's Name: Alindajao, Filoteo Diagnosis: CAD Date of Admission: Sex: 58yo Age: Male Height/WeightDocument1 pagePatient's Name: Alindajao, Filoteo Diagnosis: CAD Date of Admission: Sex: 58yo Age: Male Height/WeightButts McgeeNo ratings yet
- Hypertension Control in Asia-PacificDocument7 pagesHypertension Control in Asia-PacificNoreen Hannah GabrielNo ratings yet
- Physio Initial Assessment Form: Glasgow Coma ScaleDocument1 pagePhysio Initial Assessment Form: Glasgow Coma Scalechetha kundiNo ratings yet
- HF Secondary to HTN - Dyspnea & OrthopneaDocument3 pagesHF Secondary to HTN - Dyspnea & OrthopneaGwendolyn Talahiban LusaraNo ratings yet
- Cardiogenic Shock PathoDocument1 pageCardiogenic Shock PathoCommunity BNo ratings yet
- Republic of The Philippines Puerto Princesa City: Palawan State UniversityDocument2 pagesRepublic of The Philippines Puerto Princesa City: Palawan State UniversityRosemarie EustaquioNo ratings yet
- 4 PT Report SheetDocument1 page4 PT Report SheetAneesNo ratings yet
- CU17 CaneteDocument2 pagesCU17 CanetePrincess Laira CañeteNo ratings yet
- Super Nis Summary 2017-18Document1 pageSuper Nis Summary 2017-18api-286560136No ratings yet
- Materi - Gagal Jantung NeonatusDocument36 pagesMateri - Gagal Jantung NeonatusPutra AchmadNo ratings yet
- Ineffective Breathing Pattern Related To Shortness of Breath Possible Evidence by CuesDocument7 pagesIneffective Breathing Pattern Related To Shortness of Breath Possible Evidence by CuesLouie ParillaNo ratings yet
- Hypertension ReviewerDocument9 pagesHypertension Reviewermecleo93No ratings yet
- Coughdyspnea 2511 ArticleDocument1 pageCoughdyspnea 2511 ArticleGissele ParaisoNo ratings yet
- DR Fadillah Maricar, SPJP Angina Pectoris Dan Infark MiokardDocument50 pagesDR Fadillah Maricar, SPJP Angina Pectoris Dan Infark MiokardMuhaswadNo ratings yet
- NCP-DP NCM112LecDocument4 pagesNCP-DP NCM112LecShane CabucosNo ratings yet
- Vpomr Wodiamah EditedDocument11 pagesVpomr Wodiamah Editedsharvindan subramaniamNo ratings yet
- Pneumonia EvaluationDocument3 pagesPneumonia Evaluatione-MedTools50% (2)
- ? - Pedia MidtermsDocument18 pages? - Pedia Midtermsysabel.mendozaNo ratings yet
- 3 PT Report SheetDocument1 page3 PT Report SheetAneesNo ratings yet
- DR - Antonia Anna Lukito Slide - Webinar 18 April 2020Document34 pagesDR - Antonia Anna Lukito Slide - Webinar 18 April 2020fairuzNo ratings yet
- 2016 Update To Heart Failure Clinical Practice Guidelines: Tuesday August 2, 2016 1:00pm - 2:00pm CST (60 Minute Webinar)Document39 pages2016 Update To Heart Failure Clinical Practice Guidelines: Tuesday August 2, 2016 1:00pm - 2:00pm CST (60 Minute Webinar)Rohamonangan TheresiaNo ratings yet
- Metoprolol Drug StudyDocument4 pagesMetoprolol Drug StudyCrisha Ann Billones BacutaNo ratings yet
- Hipertensi JNC 7 VS Hipertensi JNC 8Document99 pagesHipertensi JNC 7 VS Hipertensi JNC 8Sarah Riskita MaizaliusNo ratings yet
- Agacnp 1Document29 pagesAgacnp 1academicexcellence21No ratings yet
- ViewDocument2 pagesViewJohn Lorenz OrduñaNo ratings yet
- Obesity-Ocused Physical Exam: Date - Patient InformationDocument2 pagesObesity-Ocused Physical Exam: Date - Patient InformationDem BertoNo ratings yet
- Common Abbreviations For The Patient Note USMLE Step 2CSDocument1 pageCommon Abbreviations For The Patient Note USMLE Step 2CSTiondi francisNo ratings yet
- Adult/Child: IV 2-5 Tachycardia, Anginal PainDocument10 pagesAdult/Child: IV 2-5 Tachycardia, Anginal PainKenneth Rhoel RolaNo ratings yet
- Nursing Care Plan for Pregnancy Induced HypertensionDocument2 pagesNursing Care Plan for Pregnancy Induced HypertensionTsu Wei ChuaNo ratings yet
- NURSING CARE PLAN FOR CHEST PAIN AND VOMITINGDocument2 pagesNURSING CARE PLAN FOR CHEST PAIN AND VOMITINGApril Kate BanagodosNo ratings yet
- The Importance of Potential Statin in High Risk PatientDocument56 pagesThe Importance of Potential Statin in High Risk PatientAidil Fittriani AyuNo ratings yet
- Tutorial Hipertensi IiDocument34 pagesTutorial Hipertensi Iikemuning nasutionNo ratings yet
- Hipertensão Arterial Sistêmica (HAS)Document2 pagesHipertensão Arterial Sistêmica (HAS)Suzanna LessaNo ratings yet
- 1C Dyn15 Di Florio, A - What Every CC Nurse Needs To Know ABS101Document47 pages1C Dyn15 Di Florio, A - What Every CC Nurse Needs To Know ABS101Roboschi StefaniaNo ratings yet
- Drug Study orDocument6 pagesDrug Study orAlliah MayoNo ratings yet
- Anatomy and Physiology Science Olympiad 2024 Cheat SheetDocument3 pagesAnatomy and Physiology Science Olympiad 2024 Cheat Sheetgfzmrtqj54No ratings yet
- Cardiac/Cardiogenic Shock: Clinical Practice GuidelinesDocument3 pagesCardiac/Cardiogenic Shock: Clinical Practice GuidelinesAnonymous Yo0mStNo ratings yet
- Damage - Control - Resus - Quick - Reference - Guide - Medics - Corpsmen - 2023-Quick Reference Guide For Combat Medics and CorpsmenDocument1 pageDamage - Control - Resus - Quick - Reference - Guide - Medics - Corpsmen - 2023-Quick Reference Guide For Combat Medics and Corpsmenchou youNo ratings yet
- Hanif Robbani CBD Dr. SaugiDocument29 pagesHanif Robbani CBD Dr. SaugihanifNo ratings yet
- Hypertension Concept MapDocument1 pageHypertension Concept Mapnursing concept maps100% (1)
- Nursing Care Plan For HELLP SyndromeDocument17 pagesNursing Care Plan For HELLP SyndromeRosemarie Carpio75% (4)
- Community Health Nursing and Pharmacology Course Task #4Document3 pagesCommunity Health Nursing and Pharmacology Course Task #4Michelle Angela AlombroNo ratings yet
- Stages of heart failure prevention and treatmentDocument1 pageStages of heart failure prevention and treatmentdiany astutiNo ratings yet
- Case Base Discussion: Advisor: Dr. H. M. Saugi Abduh, SP - PD, KKV, FINASIM Oleh: Muhammad Charis Mwardi (30101407246)Document53 pagesCase Base Discussion: Advisor: Dr. H. M. Saugi Abduh, SP - PD, KKV, FINASIM Oleh: Muhammad Charis Mwardi (30101407246)Aditya Reza PrianugrahaNo ratings yet
- Bright Yellow Massage BrochureDocument3 pagesBright Yellow Massage BrochurePreet PreetNo ratings yet
- Pressure ulcers are a common problem in immobile patients. Prevention and early detection are key to managementDocument72 pagesPressure ulcers are a common problem in immobile patients. Prevention and early detection are key to managementnohazz100% (2)
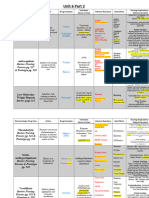
- Unit 6 Part 2 Table - Completed Fall 2023Document2 pagesUnit 6 Part 2 Table - Completed Fall 2023Tanisha SheltonNo ratings yet
- Hypertension ToolDocument2 pagesHypertension ToolPrincess AntivoNo ratings yet
- HZ SummaryDocument1 pageHZ SummaryPratzNo ratings yet
- IM-CAP Concept MapDocument1 pageIM-CAP Concept MapTrisNo ratings yet
- IM Acute Decompensation of CHF Concept MapDocument1 pageIM Acute Decompensation of CHF Concept MapTrisNo ratings yet
- DrugstudyDocument1 pageDrugstudyLorlyn OrehuelaNo ratings yet
- University of South Florida College of Nursing: Fundamental Patient Assessment ToolDocument17 pagesUniversity of South Florida College of Nursing: Fundamental Patient Assessment Toolapi-317257077No ratings yet
- CSF Production, Circulation and FunctionsDocument4 pagesCSF Production, Circulation and FunctionsAsylum AllegoryNo ratings yet
- (Bioethics 2) 2.02 - Chua-Chan - S AIDS - Health Care (Pat G)Document7 pages(Bioethics 2) 2.02 - Chua-Chan - S AIDS - Health Care (Pat G)Asylum AllegoryNo ratings yet
- (Neuro) 2.2 Seizure and Epilepsy (De Guzman&Dayrit) - Pacis&Gabasan PDFDocument7 pages(Neuro) 2.2 Seizure and Epilepsy (De Guzman&Dayrit) - Pacis&Gabasan PDFAsylum AllegoryNo ratings yet
- (Neuro) 1.1 Neurocytology (Dayrit) - JM SalesDocument4 pages(Neuro) 1.1 Neurocytology (Dayrit) - JM SalesAsylum AllegoryNo ratings yet
- (Bioethics 2) 2.02.01 - Case - Kimberly Bergalis (Pat G)Document3 pages(Bioethics 2) 2.02.01 - Case - Kimberly Bergalis (Pat G)Asylum AllegoryNo ratings yet
- 1.1 Systemic Response To InjuryDocument5 pages1.1 Systemic Response To InjuryKaren EstavilloNo ratings yet
- 3.3female and Male Genital Tract 2018Document8 pages3.3female and Male Genital Tract 2018Asylum AllegoryNo ratings yet
- Growth and development milestones in the prenatal and postnatal periodsDocument70 pagesGrowth and development milestones in the prenatal and postnatal periodsdeevoncNo ratings yet
- (Bioethics 2) 1.01 - Chua-Chan - S Human Sexuality - Responsible Parenthood (Pat G)Document4 pages(Bioethics 2) 1.01 - Chua-Chan - S Human Sexuality - Responsible Parenthood (Pat G)Asylum AllegoryNo ratings yet
- 2.3 Preventive Pediatric Medicine Part 3Document7 pages2.3 Preventive Pediatric Medicine Part 3Asylum AllegoryNo ratings yet
- 3.1 Applied Lecture - Pediatric History - BahaghariDocument5 pages3.1 Applied Lecture - Pediatric History - BahaghariAsylum AllegoryNo ratings yet
- 3.2 Applied Lecture - Neonatal History - BahaghariDocument6 pages3.2 Applied Lecture - Neonatal History - BahaghariAsylum AllegoryNo ratings yet
- 2.3 Preventive Pediatric Medicine Part 1Document5 pages2.3 Preventive Pediatric Medicine Part 1Asylum AllegoryNo ratings yet
- 2.3 Preventive Pediatric Medicine Part 4Document6 pages2.3 Preventive Pediatric Medicine Part 4Asylum AllegoryNo ratings yet
- 3.1 Applied Lecture - Pediatric History - BahaghariDocument5 pages3.1 Applied Lecture - Pediatric History - BahaghariAsylum AllegoryNo ratings yet
- 2.2 Breastfeeding and Malnutrition - Bahaghari TransDocument9 pages2.2 Breastfeeding and Malnutrition - Bahaghari TransAsylum AllegoryNo ratings yet
- 2.3 Preventive Pediatric Medicine Part 2Document6 pages2.3 Preventive Pediatric Medicine Part 2Asylum AllegoryNo ratings yet
- Comorbidity Clusters Associated With Newly Treated Type 2 Diabetes Mellitus - A Bayesian Nonparametric AnalysisDocument13 pagesComorbidity Clusters Associated With Newly Treated Type 2 Diabetes Mellitus - A Bayesian Nonparametric AnalysisShayekh M ArifNo ratings yet
- Special Collection ProceduresDocument6 pagesSpecial Collection ProceduresB12 Clifford GarciaNo ratings yet
- 1940 12050 1 PBDocument7 pages1940 12050 1 PBmano mayNo ratings yet
- 4 Blood Physiology (FINAL)Document8 pages4 Blood Physiology (FINAL)kath-kathNo ratings yet
- Electrolytes Water Balance PH Balance Trace MetalsDocument21 pagesElectrolytes Water Balance PH Balance Trace MetalsJohn Kevin Carl SaligumbaNo ratings yet
- NF) S ) JF Cfof) U G) Kfn:Jf:Yo ) JF, HG/N GL (Ë D"X, Xfos KFFRF) + Tx,:6Fkm G (KBSF) V'NNF / CFGTL/S K - Ltof) Lutftds LNLVT K/Liffsf) Kf7/OqmdDocument4 pagesNF) S ) JF Cfof) U G) Kfn:Jf:Yo ) JF, HG/N GL (Ë D"X, Xfos KFFRF) + Tx,:6Fkm G (KBSF) V'NNF / CFGTL/S K - Ltof) Lutftds LNLVT K/Liffsf) Kf7/OqmdAnil BasnetNo ratings yet
- Vasopressor & InotropesDocument44 pagesVasopressor & InotropesArun KumarNo ratings yet
- BISOMET STUDY COMPARES BISOPROLOL AND METOPROLOLDocument5 pagesBISOMET STUDY COMPARES BISOPROLOL AND METOPROLOLSamayanaboyana BabuNo ratings yet
- Thoat ENT D&R AgamDocument231 pagesThoat ENT D&R AgamRobb StarkNo ratings yet
- Sample Health HistoryDocument2 pagesSample Health HistoryDagmawi BahiruNo ratings yet
- Clinical ElectrocardiographyDocument134 pagesClinical ElectrocardiographyHossain MuhammadNo ratings yet
- The Effects of Exercise Training in Adult Solid Organ Transplant Recipients A Systematic Review and Meta-AnalysisDocument24 pagesThe Effects of Exercise Training in Adult Solid Organ Transplant Recipients A Systematic Review and Meta-AnalysisJesusNavarrete97No ratings yet
- Monogenic Diabetes (MGD) : Modyand OthersDocument62 pagesMonogenic Diabetes (MGD) : Modyand Othersسالم عبداللهNo ratings yet
- Pleural EffusionDocument49 pagesPleural EffusionLyra Lorca86% (7)
- FCPS Pretest Golden File 1Document450 pagesFCPS Pretest Golden File 1Khadija AurangzebNo ratings yet
- Aortic Aneurysm Info From Mass GeneralDocument8 pagesAortic Aneurysm Info From Mass Generalclubsingr28No ratings yet
- Biochemistry "Lipids Test"Document8 pagesBiochemistry "Lipids Test"HERONo ratings yet
- (GERIA) Quiz 1Document11 pages(GERIA) Quiz 1Charmaine AmagoNo ratings yet
- Thorax - OverviewDocument5 pagesThorax - OverviewAlfNo ratings yet
- Eye Docs GlaucomaDocument147 pagesEye Docs GlaucomaMuneeb ShahzadNo ratings yet
- Science 9 ReviewerDocument22 pagesScience 9 ReviewerRio OrpianoNo ratings yet
- Article - Billing and Coding - Non-Invasive Peripheral Arterial Vascular Studies (A57593)Document33 pagesArticle - Billing and Coding - Non-Invasive Peripheral Arterial Vascular Studies (A57593)Michael Lopez OlivaNo ratings yet
- Hyponatremia Sah 1Document13 pagesHyponatremia Sah 1RA Tri Retno WulanNo ratings yet
- Basinger Abraham - ConsultationDocument80 pagesBasinger Abraham - ConsultationVikas NairNo ratings yet
- Acute Coronary SyndromeDocument9 pagesAcute Coronary SyndromeAnthony Philip Patawaran CalimagNo ratings yet
- Anaemia in Pregnancy GuideDocument33 pagesAnaemia in Pregnancy GuideKomal Dhulap100% (1)
- Sarawak Handbook of Medical Emergencies, 3rd EdDocument410 pagesSarawak Handbook of Medical Emergencies, 3rd EdKelvin SuNo ratings yet
- Chapter 9 CARDIOVASCULAR SYSTEMDocument21 pagesChapter 9 CARDIOVASCULAR SYSTEMAlexander Santiago ParelNo ratings yet
- Anatomy and Pathology of The Eye: Role of MR Imaging and CTDocument25 pagesAnatomy and Pathology of The Eye: Role of MR Imaging and CTCucută Alexandru-DanielNo ratings yet
- NearfatalasthmaDocument8 pagesNearfatalasthmaHeath HensleyNo ratings yet