You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
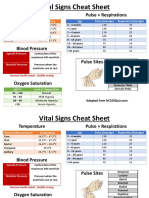
- Vital Signs Cheat Sheet Guide Ranges Temps Pulses RespirationsDocument2 pagesVital Signs Cheat Sheet Guide Ranges Temps Pulses RespirationsMarshin Thea Celocia100% (1)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Surgery MnemonicsDocument4 pagesSurgery MnemonicsMark Anthony Namoca100% (1)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Anatomy Mnemonics 2Document50 pagesAnatomy Mnemonics 2Nourhan JamalNo ratings yet
- Amaurosis FugaxDocument11 pagesAmaurosis FugaxRexArtem100% (1)
- 1 - Anatomy of The KidneyDocument15 pages1 - Anatomy of The Kidneysara khanNo ratings yet
- Google Doc - Mark K NCLEX Study GuideDocument62 pagesGoogle Doc - Mark K NCLEX Study Guideezinne obinna-umaNo ratings yet
- EUOGS OSCE Booklet 2020Document26 pagesEUOGS OSCE Booklet 2020Amanda Leow100% (1)
- Anatomy of Thorax Mbbs CXRDocument55 pagesAnatomy of Thorax Mbbs CXRMehtab AhmadNo ratings yet
- Eosinophil Biology and Causes of Eosinophilia - UpToDateDocument35 pagesEosinophil Biology and Causes of Eosinophilia - UpToDateBls PriyaNo ratings yet
- COVID-19 Quiz Review for Nurses: Coronavirus Symptoms, Transmission & PreventionDocument11 pagesCOVID-19 Quiz Review for Nurses: Coronavirus Symptoms, Transmission & Preventionhasan ahmdNo ratings yet
- ECase 08 - Tutorial 1 - 2021 Josh ThomasDocument15 pagesECase 08 - Tutorial 1 - 2021 Josh ThomasjoshNo ratings yet
- Sample Medical ReportsDocument6 pagesSample Medical ReportsMayNo ratings yet
- Conduct of Physical Examination RemindersDocument23 pagesConduct of Physical Examination RemindersJazer DairoNo ratings yet
- Drug CalculationDocument34 pagesDrug CalculationMalathi VarnaNo ratings yet
- Pericardial DiseseasDocument38 pagesPericardial Diseseasmameekasim75No ratings yet
- Jurnal Code BlueDocument4 pagesJurnal Code BlueHusnul KeenNo ratings yet
- SaludDocument16 pagesSaluddianamera84No ratings yet
- College of Health Sciences: Urdaneta City UniversityDocument4 pagesCollege of Health Sciences: Urdaneta City UniversityBianca Marithè RejanoNo ratings yet
- Combivent Nursing ResponsibilitiesDocument2 pagesCombivent Nursing ResponsibilitiesGwyn RosalesNo ratings yet
- Blood VesselsDocument43 pagesBlood VesselsJessica AcostaNo ratings yet
- Resep IbuprofenDocument8 pagesResep Ibuprofen27. SYAHRIN AZRIL IZULKHAQUENo ratings yet
- Intrauterine Growth RestrictionDocument26 pagesIntrauterine Growth RestrictionrajaeasNo ratings yet
- College Nursing Drug RecordDocument12 pagesCollege Nursing Drug RecordJae TyNo ratings yet
- Dose of Jogging and Long-Term Mortality: The Copenhagen City Heart StudyDocument9 pagesDose of Jogging and Long-Term Mortality: The Copenhagen City Heart StudyCharles SeekNo ratings yet
- Apixaban Vs ASA en Ictus Embólico de Fuente IndeterminadaDocument12 pagesApixaban Vs ASA en Ictus Embólico de Fuente IndeterminadaOscar SantosNo ratings yet
- Online Cardiologist Consultation - Connect2mydoctorDocument12 pagesOnline Cardiologist Consultation - Connect2mydoctorKrishna PrasadNo ratings yet
- Gestational HypertensionDocument2 pagesGestational HypertensionReyniel Pablo ElumbaNo ratings yet
- Intermediate Care Units Recommendations On Facilities and StructureDocument12 pagesIntermediate Care Units Recommendations On Facilities and StructureJHNo ratings yet
- Lippincott Pathology QuestionsDocument10 pagesLippincott Pathology Questionsابواحمد المجاهدNo ratings yet
- Cardio Notes 1Document8 pagesCardio Notes 1Lindsay Grace MandarioNo ratings yet