You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Clinical Practice Guideline: Tympanostomy Tubes in Children (Update)Document56 pagesClinical Practice Guideline: Tympanostomy Tubes in Children (Update)anitaabreu123No ratings yet
- DHA Past PapersDocument153 pagesDHA Past Papersamolkupwad100% (3)
- Jurnal Adhesive Otitis MediaDocument18 pagesJurnal Adhesive Otitis MediaJimmy ChuaNo ratings yet
- Otitis MediaDocument4 pagesOtitis MediaapocruNo ratings yet
- Ent-Mcq-C2 426Document7 pagesEnt-Mcq-C2 426Sheikha100% (5)
- Easy Peasy EardrumsDocument52 pagesEasy Peasy EardrumsUCD GEMNo ratings yet
- Cod Liver Oil - Setting The Record Straight - The Weston A. Price FoundationDocument5 pagesCod Liver Oil - Setting The Record Straight - The Weston A. Price FoundationRicardo BritoNo ratings yet
- Original Article: Wasif Siddique, Abdul Hakeem, Kamran Ashfaq, Maryam Khan, Asif Alam GulDocument5 pagesOriginal Article: Wasif Siddique, Abdul Hakeem, Kamran Ashfaq, Maryam Khan, Asif Alam GulGalvin GiffariNo ratings yet
- ENT MCQsDocument13 pagesENT MCQsSheikha100% (2)
- Nursing Practice II 2010Document16 pagesNursing Practice II 2010Anonymous NnC87DtzQNo ratings yet
- Patulous Eustachian Tube (Pet), A Practical: SciencedirectDocument6 pagesPatulous Eustachian Tube (Pet), A Practical: SciencedirectLimeysahni NazhoeNo ratings yet
- ENT Care For MO - ENT Care, WHY & WHEREDocument62 pagesENT Care For MO - ENT Care, WHY & WHEREsanmukh chawlaNo ratings yet
- ENT ESSAYS: Guide to Ear, Nose & Throat ConditionsDocument78 pagesENT ESSAYS: Guide to Ear, Nose & Throat ConditionsNektarios Tsakalos100% (1)
- Functional analysis of episodic self-injury linked to ear infectionsDocument3 pagesFunctional analysis of episodic self-injury linked to ear infectionsTimiNo ratings yet
- Answer Key Intraboard BDocument14 pagesAnswer Key Intraboard BJonas Marvin Anaque100% (3)
- Endoscopic Insertion of Tympanostomy Tube in Children: Aso Nuri Jalizada, Mouwafaq Al Rawi, Lana Abdul Razzaq DabbaghDocument5 pagesEndoscopic Insertion of Tympanostomy Tube in Children: Aso Nuri Jalizada, Mouwafaq Al Rawi, Lana Abdul Razzaq DabbaghSucii Sekar NingrumNo ratings yet
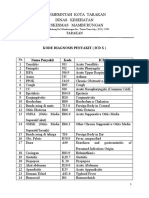
- Pemerintah Kota Tarakan Dinas Kesehatan Puskesmas MamburunganDocument3 pagesPemerintah Kota Tarakan Dinas Kesehatan Puskesmas MamburunganHairulNo ratings yet
- Pediatric Respiratory Cases: DR Hodan S. Ahmed, Department of Pediatrics and Child Health, Amoud Medical School, AUDocument24 pagesPediatric Respiratory Cases: DR Hodan S. Ahmed, Department of Pediatrics and Child Health, Amoud Medical School, AUmukhtar abddiNo ratings yet
- 6-7 Omsk MalignaDocument2 pages6-7 Omsk MalignaAlvina Ulfah RusmayuniNo ratings yet
- Cap. 12. ENT DISORDERS PDFDocument10 pagesCap. 12. ENT DISORDERS PDFoana policarpov100% (1)
- Kode Simpus PTT EMIDocument18 pagesKode Simpus PTT EMIfauziahNo ratings yet
- Assessment and Management of Patients With Hearing and Balance DisordersDocument9 pagesAssessment and Management of Patients With Hearing and Balance Disordersxhemhae100% (1)
- Clinical Evaluation Summaries for Headaches and Eye IssuesDocument6 pagesClinical Evaluation Summaries for Headaches and Eye IssuesPrincess MarielleNo ratings yet
- Jurnal Mastoid Abscess in Acute and Chronic Otitis Media PDFDocument7 pagesJurnal Mastoid Abscess in Acute and Chronic Otitis Media PDFRichard SimakNo ratings yet
- Joette CalabreseDocument29 pagesJoette Calabresenaveen kumarNo ratings yet
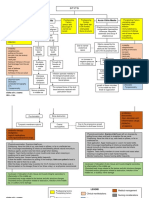
- OTITIS Concept MapDocument7 pagesOTITIS Concept MapElleNo ratings yet
- Ent MCQ A.pfdDocument61 pagesEnt MCQ A.pfdSuresh Kumar Bansal90% (10)
- Section H. Morbidity Diseases Report: Rhu IDocument6 pagesSection H. Morbidity Diseases Report: Rhu ITiffany SalalimaNo ratings yet
- Current Concepts in The Pathogenesis and Treatment of Chronic Suppurative Otitis MediaDocument14 pagesCurrent Concepts in The Pathogenesis and Treatment of Chronic Suppurative Otitis MediaKoko AgungNo ratings yet
- Master Tung's Four Horses Combination - Master Tung's Magic PointsDocument12 pagesMaster Tung's Four Horses Combination - Master Tung's Magic PointsAWEDIOHEAD93% (14)