You might also like
- Agents Used To Treat Hyperuricemia and GoutDocument19 pagesAgents Used To Treat Hyperuricemia and GoutQuolette Constante100% (1)
- 13 Antacids and ControllersDocument51 pages13 Antacids and ControllersDennis Nabor Muñoz, RN,RMNo ratings yet
- Agents Used To Treat Gastrointestinal DisordersDocument53 pagesAgents Used To Treat Gastrointestinal DisordersQuolette ConstanteNo ratings yet
- Opioid AnalgesicsDocument44 pagesOpioid AnalgesicsQuolette ConstanteNo ratings yet
- Adrenergic BlockersDocument71 pagesAdrenergic BlockersCodered Review100% (1)
- Antiinflammatory Agents and Nonsteroidal Antiinflammatory Drugs (Nsaids)Document26 pagesAntiinflammatory Agents and Nonsteroidal Antiinflammatory Drugs (Nsaids)Codered ReviewNo ratings yet
- Bronchodilators and Other Respiratory AgentsDocument47 pagesBronchodilators and Other Respiratory AgentsQuolette ConstanteNo ratings yet
- CNS DepressantsDocument27 pagesCNS DepressantsCodered ReviewNo ratings yet
- 04 Cholinergic Blockers UpdDocument58 pages04 Cholinergic Blockers Updakazukin002100% (1)
- Drugs Affecting The Respiratory SystemDocument61 pagesDrugs Affecting The Respiratory SystemQuolette ConstanteNo ratings yet
- 18 Antivirals UpdDocument19 pages18 Antivirals Updakazukin002100% (4)
- CancerDocument81 pagesCancerCodered Review100% (1)
- Antimalarial, Antiprotozoal, and Antihelmintic AgentsDocument37 pagesAntimalarial, Antiprotozoal, and Antihelmintic AgentsQuolette ConstanteNo ratings yet
- Antifungal AgentsDocument22 pagesAntifungal AgentsQuolette Constante100% (1)
- 17 AntibioticsDocument67 pages17 AntibioticsQuolette ConstanteNo ratings yet
- Lecture 23 - The Urinary SystemDocument46 pagesLecture 23 - The Urinary SystemIhab MoustafaNo ratings yet
- Psychitaric and Mental Health NursingDocument9 pagesPsychitaric and Mental Health NursingCodered ReviewNo ratings yet
- JurisprudenceDocument55 pagesJurisprudenceCodered ReviewNo ratings yet
- Perioperative NursingDocument271 pagesPerioperative NursingCodered Review100% (3)
- Alteration in The Immune ResponseDocument42 pagesAlteration in The Immune ResponseCodered ReviewNo ratings yet
- Anatomy and PhysiologyDocument288 pagesAnatomy and PhysiologyCodered ReviewNo ratings yet
- Metabolism: Endocrine SystemDocument129 pagesMetabolism: Endocrine SystemCodered Review100% (1)
- List of PassersDocument751 pagesList of PassersJeanhel AuditorNo ratings yet
- PINOYBSNJuly 2011 Nursing Board Exam Result Top Performing SchoolsDocument19 pagesPINOYBSNJuly 2011 Nursing Board Exam Result Top Performing Schoolspinoybsn1192No ratings yet
- List of PassersDocument751 pagesList of PassersJeanhel AuditorNo ratings yet
- July 2011 Nursing Board Exam Top 10 Successful ExamineesDocument2 pagesJuly 2011 Nursing Board Exam Top 10 Successful ExamineesPhilippineNursingDirectory.comNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- DHPL Equipment Updated List Jan-22Document16 pagesDHPL Equipment Updated List Jan-22jairamvhpNo ratings yet
- 2JA5K2 FullDocument22 pages2JA5K2 FullLina LacorazzaNo ratings yet
- How To Make Money in The Stock MarketDocument40 pagesHow To Make Money in The Stock Markettcb66050% (2)
- BRD TemplateDocument4 pagesBRD TemplateTrang Nguyen0% (1)
- 2022 Product Catalog WebDocument100 pages2022 Product Catalog WebEdinson Reyes ValderramaNo ratings yet
- API MidtermDocument4 pagesAPI MidtermsimranNo ratings yet
- Chill - Lease NotesDocument19 pagesChill - Lease Notesbellinabarrow100% (4)
- Tech Letter-NFPA 54 To Include Bonding 8-08Document2 pagesTech Letter-NFPA 54 To Include Bonding 8-08gl lugaNo ratings yet
- Binaural Recording Technology: A Historical Review and Possible Future DevelopmentsDocument22 pagesBinaural Recording Technology: A Historical Review and Possible Future DevelopmentsNery BorgesNo ratings yet
- MN AG v. SANOFI - 3:18-cv-14999 - Defendants' Joint Motion To Dismiss - 2019-08-12Document124 pagesMN AG v. SANOFI - 3:18-cv-14999 - Defendants' Joint Motion To Dismiss - 2019-08-12The Type 1 Diabetes Defense FoundationNo ratings yet
- CSEC IT Fundamentals of Hardware and SoftwareDocument2 pagesCSEC IT Fundamentals of Hardware and SoftwareR.D. Khan100% (1)
- Introduction To Elective DesignDocument30 pagesIntroduction To Elective Designabdullah 3mar abou reashaNo ratings yet
- Module 5Document10 pagesModule 5kero keropiNo ratings yet
- Civil Aeronautics BoardDocument2 pagesCivil Aeronautics BoardJayson AlvaNo ratings yet
- Dwnload Full International Monetary Financial Economics 1st Edition Daniels Solutions Manual PDFDocument36 pagesDwnload Full International Monetary Financial Economics 1st Edition Daniels Solutions Manual PDFelegiastepauleturc7u100% (16)
- Berry B Brey Part IDocument49 pagesBerry B Brey Part Ikalpesh_chandakNo ratings yet
- EWAIRDocument1 pageEWAIRKissy AndarzaNo ratings yet
- Group 4-Hospital Information System - His - QuizDocument2 pagesGroup 4-Hospital Information System - His - QuizGeeyan Marlchest B NavarroNo ratings yet
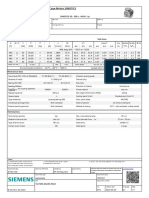
- 1LE1503-2AA43-4AA4 Datasheet enDocument1 page1LE1503-2AA43-4AA4 Datasheet enAndrei LupuNo ratings yet
- Diana's Innermost House: MagazineDocument42 pagesDiana's Innermost House: MagazinealexgoagaNo ratings yet
- 3 Course Contents IIIBDocument5 pages3 Course Contents IIIBshahabNo ratings yet
- Instrumentos de Medición y Herramientas de Precisión Starrett DIAl TEST INDICATOR 196 A1ZDocument24 pagesInstrumentos de Medición y Herramientas de Precisión Starrett DIAl TEST INDICATOR 196 A1Zmicmarley2012No ratings yet
- Okuma Osp5000Document2 pagesOkuma Osp5000Zoran VujadinovicNo ratings yet
- Mini Ice Plant Design GuideDocument4 pagesMini Ice Plant Design GuideDidy RobotIncorporatedNo ratings yet
- Diagnostic Information For Database Replay IssuesDocument10 pagesDiagnostic Information For Database Replay IssuesjjuniorlopesNo ratings yet
- Tata Group's Global Expansion and Business StrategiesDocument23 pagesTata Group's Global Expansion and Business Strategiesvgl tamizhNo ratings yet
- Unit 1 2marksDocument5 pagesUnit 1 2marksLokesh SrmNo ratings yet
- Aci 207.1Document38 pagesAci 207.1safak kahraman100% (7)
- Developing a Positive HR ClimateDocument15 pagesDeveloping a Positive HR ClimateDrPurnima SharmaNo ratings yet
- Cercado VsDocument1 pageCercado VsAnn MarieNo ratings yet