You might also like
- Frozen Shoulder ExercisesDocument2 pagesFrozen Shoulder ExercisesUsman MalikNo ratings yet
- CVA - IE This Is ItDocument33 pagesCVA - IE This Is ItJen PassilanNo ratings yet
- Gait FESDocument11 pagesGait FESJen PassilanNo ratings yet
- Copy (2) of Mavic ElectroDocument8 pagesCopy (2) of Mavic ElectroJen PassilanNo ratings yet
- Copy (2) of Mavic ElectroDocument8 pagesCopy (2) of Mavic ElectroJen PassilanNo ratings yet
- Aerobic Exercises 2Document71 pagesAerobic Exercises 2Jen Passilan100% (1)
- EmphysemaDocument60 pagesEmphysemaJen Passilan100% (6)
- MethodsDocument11 pagesMethodsJen PassilanNo ratings yet
- ThoraxDocument67 pagesThoraxJen PassilanNo ratings yet
- Muscle CrampsDocument40 pagesMuscle CrampsJen Passilan100% (2)
- Copy (2) of Mavic ElectroDocument8 pagesCopy (2) of Mavic ElectroJen PassilanNo ratings yet
- Manual TherapyDocument87 pagesManual TherapyJen Passilan100% (9)
- Regulation of Cardiac FXN - ECGDocument71 pagesRegulation of Cardiac FXN - ECGJen PassilanNo ratings yet
- Spinal Cord Injury - CompleteDocument88 pagesSpinal Cord Injury - CompleteJen Passilan100% (10)
- The Gross Appearance of Spinal Cord-Lec by EmmaDocument32 pagesThe Gross Appearance of Spinal Cord-Lec by EmmaJen Passilan100% (1)
- CrampsDocument14 pagesCrampsJen PassilanNo ratings yet
- Spinal CordDocument13 pagesSpinal CordJen PassilanNo ratings yet
- Spinal Cord Injury (SCI)Document10 pagesSpinal Cord Injury (SCI)Jen PassilanNo ratings yet
- Balance & Mobility Following Stroke: Effects of Physical Therapy Interventions With & WithoutDocument38 pagesBalance & Mobility Following Stroke: Effects of Physical Therapy Interventions With & WithoutJen PassilanNo ratings yet
- Reproductive LectureDocument89 pagesReproductive LectureJen PassilanNo ratings yet
- PT Management of Spinal Cord InjuryDocument20 pagesPT Management of Spinal Cord InjuryJen Passilan100% (1)
- Diagnostic Examinations & ToolsDocument25 pagesDiagnostic Examinations & ToolsJen PassilanNo ratings yet
- JournalDocument34 pagesJournalJen PassilanNo ratings yet
- Digestive SystemDocument43 pagesDigestive SystemJen PassilanNo ratings yet
- MethodsDocument11 pagesMethodsJen PassilanNo ratings yet
- Balance & Mobility Following Stroke: Effects of Physical Therapy Interventions With & WithoutDocument38 pagesBalance & Mobility Following Stroke: Effects of Physical Therapy Interventions With & WithoutJen PassilanNo ratings yet
- HeartDocument51 pagesHeartJen PassilanNo ratings yet
- Balance & Mobility Following Stroke: Effects of Physical Therapy Interventions With & WithoutDocument38 pagesBalance & Mobility Following Stroke: Effects of Physical Therapy Interventions With & WithoutJen PassilanNo ratings yet
- ArrhythmiasDocument23 pagesArrhythmiasJen PassilanNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- 'Rrlyry: Ba) LRTDocument8 pages'Rrlyry: Ba) LRTMunish KumarNo ratings yet
- How To Stop SmokingDocument43 pagesHow To Stop SmokingRoselyn PacardoNo ratings yet
- Consultant Job Planning Diary V 63Document10 pagesConsultant Job Planning Diary V 63محمدعلیجبارNo ratings yet
- January 8, 2018: Author: Lily Dong, SIRCDocument5 pagesJanuary 8, 2018: Author: Lily Dong, SIRCshirwen ClamNo ratings yet
- Clinical Tips in Cardiovascular EmergenciesDocument86 pagesClinical Tips in Cardiovascular EmergenciesAbdul Quyyum100% (3)
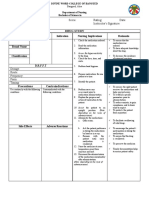
- Drug Study NCP Template 2Document2 pagesDrug Study NCP Template 2Janico Lanz BernalNo ratings yet
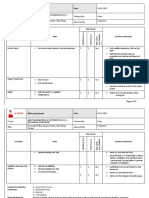
- Risk Assessment - AbbDocument3 pagesRisk Assessment - AbbAbdul RaheemNo ratings yet
- Quality Function Deployment in HealthcareDocument14 pagesQuality Function Deployment in HealthcareMarvi HarsiNo ratings yet
- Occupational Health and Safety - 2Document4 pagesOccupational Health and Safety - 2Kero KeropiNo ratings yet
- Volkmann's Ischemic Contracture by Innocent C. AbuguDocument38 pagesVolkmann's Ischemic Contracture by Innocent C. AbuguChukwuemeka ChidogoNo ratings yet
- Breastfeeding Issues, RX If Mother N Baby in HivDocument82 pagesBreastfeeding Issues, RX If Mother N Baby in HivMallika JoonNo ratings yet
- Julia Harwood Promoted To Senior Vice President of Clinical Operations For New York Cancer & Blood SpecialistsDocument3 pagesJulia Harwood Promoted To Senior Vice President of Clinical Operations For New York Cancer & Blood SpecialistsPR.comNo ratings yet
- Group DR - Script - Allergic Rhinitis (Peanut Allergy) Health EducationDocument10 pagesGroup DR - Script - Allergic Rhinitis (Peanut Allergy) Health EducationKyra Bianca R. FamacionNo ratings yet
- Brain On Food: This Is YourDocument2 pagesBrain On Food: This Is YourMuralidhar Rao ShintreNo ratings yet
- 1 PBDocument10 pages1 PBKenny ZefanyaNo ratings yet
- Omeprazole drug studyDocument3 pagesOmeprazole drug studyNadeen Fariscal100% (1)
- BJSTR MS Id 004577Document8 pagesBJSTR MS Id 004577SartajHussainNo ratings yet
- ILO Brief: ILO Violence and Harassment Convention, 2019 (No. 190)Document4 pagesILO Brief: ILO Violence and Harassment Convention, 2019 (No. 190)Zebi Magnolia FawwazNo ratings yet
- Contemporary Professional NursingDocument18 pagesContemporary Professional NursingAamirNo ratings yet
- Thyroid History and Physical Examination Key PointsDocument49 pagesThyroid History and Physical Examination Key PointsAbeer RadiNo ratings yet
- BD Contact Information: BD Global Product Incident Report (Pir) Form 1501-092-011-RDocument2 pagesBD Contact Information: BD Global Product Incident Report (Pir) Form 1501-092-011-RrsuertoNo ratings yet
- 3 s2.0 B9781455748013003301 MainDocument120 pages3 s2.0 B9781455748013003301 MainInzamam Ul HaqNo ratings yet
- Lesson 07 Listeriosis - Bacterial Infection From Listeria Monocytogenes PDFDocument4 pagesLesson 07 Listeriosis - Bacterial Infection From Listeria Monocytogenes PDFGwendolyn CalatravaNo ratings yet
- Approach To Differential Diagnosis PDFDocument62 pagesApproach To Differential Diagnosis PDFanasNo ratings yet
- Ch6 ImmuneDocument49 pagesCh6 ImmuneleartaNo ratings yet
- Risk assessment form for painting workDocument1 pageRisk assessment form for painting workNarender BhardwajNo ratings yet
- National Annual Review 2073/74: Central HospitalsDocument20 pagesNational Annual Review 2073/74: Central HospitalsAtul KumarNo ratings yet
- Health Promotion Stress Management AssignmentDocument10 pagesHealth Promotion Stress Management Assignmentapi-211472021No ratings yet
- Prevalence of Stress and Its Association With Resilience Among Medical Students in A Tertiary Care Center, Aurangabad, Maharashtra, IndiaDocument9 pagesPrevalence of Stress and Its Association With Resilience Among Medical Students in A Tertiary Care Center, Aurangabad, Maharashtra, IndiaIJAR JOURNALNo ratings yet
- Bacls PDFDocument23 pagesBacls PDFAngelo Domingo0% (1)